It is important that your medical practitioner, whether physician or physiotherapist does his own evidence based objective examinations. This allows efficacious evidence-based treatment arising from clinical examination.
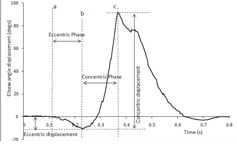
Together with a series of questions in the subjective examination, the objective examination allows specific testing the ability to come to a specific diagnosis, either through a process of exclusion or positive tests.
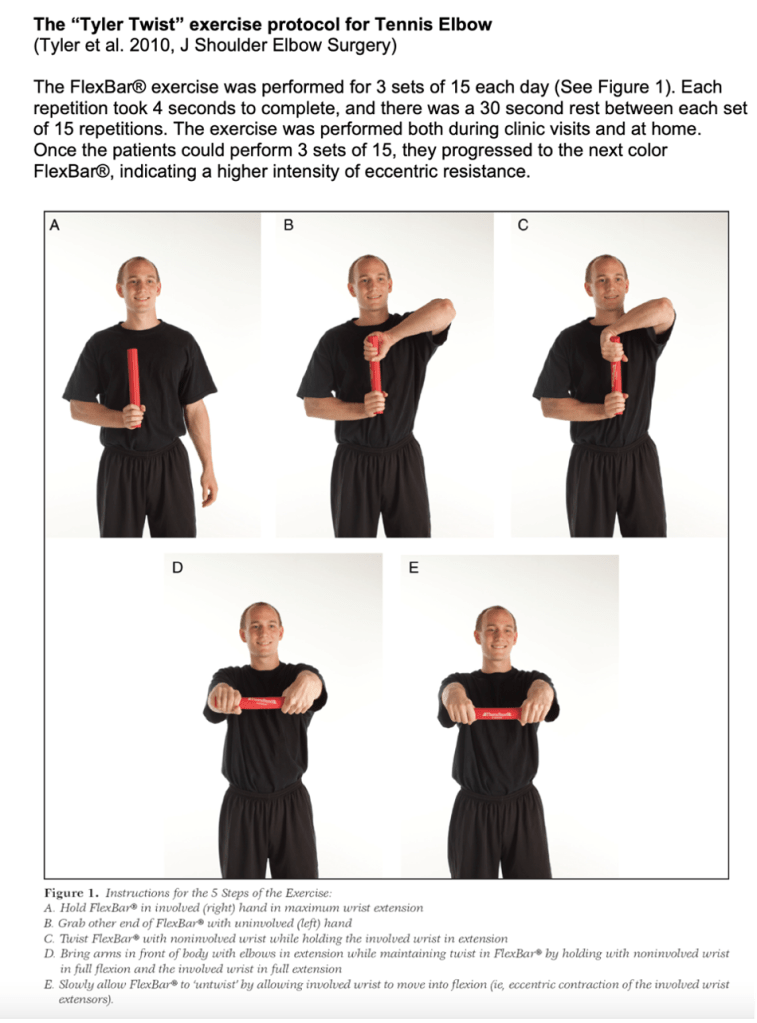
Special tests for Lateral Epicndylitis (Tennis Elbow):
(MacDermid and Michlovitz, 2006)
Treatment strategies:
Ice & compression; Mobilistions, Trigger point therapy. Exercise therapy based on limitations and weaknesses identified in physical examination. Muligan accessory movements and mobilisations can show efficacy (Abbott et al., 2001).
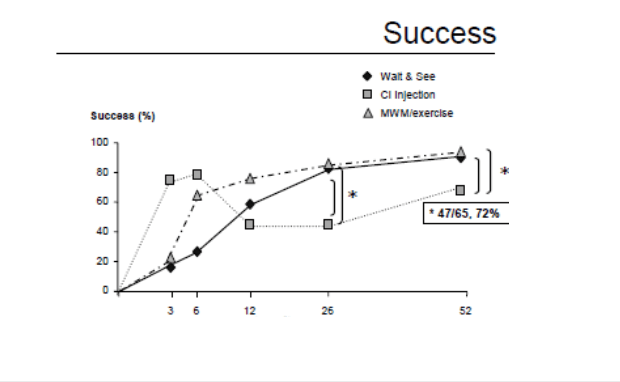
Corticosteroids which is a mainstay of many treatment protocols have very little long-term success. In fact, the results are worse. As can be seen in the chart below, Corticosteroid injections had worse results that both wait and see approaches as well as Mobilisations and exercise treatment protocol (Bisset et al., 2006). The literature is showing that these injections should no longer be used in this condition.
(Bisset et al., 2006)
Anothr Meta-analysis in 2010 also showed worse results from steroid use as compared to other treatments in both the intermediate and long term (Coombes et al., 2010).
Surgical intervention is rserved for those who remain symptomatic for greater than 6 month. Reccurance and chronic condition may be considered for surgery. People with larger tears were also more likely to have inefficient conservative treatment (Clarke, 2010 #389).
ABBOTT, J. H., PATLA, C. E. & JENSEN, R. H. 2001. The initial effects of an elbow mobilization with movement technique on grip strength in subjects with lateral epicondylalgia. Man Ther, 6, 163-9.
BISSET, L., BELLER, E., JULL, G., BROOKS, P., DARNELL, R. & VICENZINO, B. 2006. Mobilisation with movement and exercise, corticosteroid injection, or wait and see for tennis elbow: randomised trial. Bmj, 333, 939.
COOMBES, B. K., BISSET, L. & VICENZINO, B. 2010. Efficacy and safety of corticosteroid injections and other injections for management of tendinopathy: a systematic review of randomised controlled trials. Lancet, 376, 1751-67.
MACDERMID, J. C. & MICHLOVITZ, S. L. 2006. Examination of the elbow: linking diagnosis, prognosis, and outcomes as a framework for maximizing therapy interventions. J Hand Ther, 19, 82-97.
TYLER, T. F., THOMAS, G. C., NICHOLAS, S. J. & MCHUGH, M. P. 2010. Addition of isolated wrist extensor eccentric exercise to standard treatment for chronic lateral epicondylosis: a prospective randomized trial. J Shoulder Elbow Surg, 19, 917-22.
There is significant disagreement between much of the literature with regards to the management of adolescent idiopathic scoliosis and to the efficacy of exercise intervention in establishing a meaningful long-term outcome. On the one hand many longitudinal studies are showing many physical therapies as not changing the eventual long-term prognosis of the condition. Yet there is also simultaneously a lot of literature on the efficacy of exercise on multiple measures showing categoric improvements on health and quality of life. Specific scoliosis intervention protocols Physiotherapeutic Scoliosis-Specific Exercises
(PSSE’s) have shown significant Cobb angle reduction, of up to a year follow up (1). Modalities that include PSSE re-education of postural alignment include methods such as “Dobomed, FITS, Lyon, Schroth, SEAS and side shift” (2).
The most common form of scoliosis is adolescent idiopathic scoliosis. A 50-year follow-up study on late-onset idiopathic scoliosis showed that 117 untreated patients and 62 age/sex matched volunteers found that patients with untreated scoliosis are, productive, high functioning and usually have little physical impairment other than back pain and cosmetic concerns. (3) Three major factors for progression include, magnitude of curve on presentation and growth potential as well as sex. Initial Cobb angle magnitude was the most important predictor of long-term curve progression. Sex, initial age and pubertal status were less important predictors. An initial Cobb angle of 25 degrees was an important threshold for predictive long-term progression (4). Growth potential is based on age and tanner stage, more precisely with radiographs for Risser grade, measuring bony fusion of iliac apophysis (5). Risk progression increases with higher Cobb and lower Risser Grade. A review by Reamy et. al (2001), concludes that physical therapy, chiropractic care, biofeedback and electric stimulation have not been shown to alter the natural history of scoliosis (6). In contrast bracing and spinal surgery at the required progression of the scoliosis and Cobb angle have shown efficacy as reported by Reamy et al. (2001). (6)
A review in 2005 indicates less need for radiographs, as it does not necessarily influence treatment protocol (7). An umbrella review of the literature in 2014 based on best evidence concludes that there were several systematic reviews that were scored as ‘moderate to low quality’ between 2002 and 2011. Indeed the 2012 US Preventative Service Task Force recommendation against screening was based on a low quality 2004 review (8). Plaszewski (2014) concludes that the suggestion for less screening is based on papers older that 10 years old and therefore outdated, and more importantly they did not review the methodological quality of these papers of which they included in their reviews. (8)
One such paper that claimed bracing and surgical intervention were the only route that made a difference, was cited by a 1988 study (9) as a locum of evidence for a study written in 2001 (Reference: 9) (6). More primary studies are therefore needed to methodologically assess the efficacy of screening as of 2014 (8).
Indeed, studies as early as 2003 have been criticising much of the literature against exercise intervention in the progression of scoliosis. Hawes (2003) concludes emphatically that there is not a single decisive study that mandates early exercise intervention of scoliosis is of no use (10). It is already known that given the known risks of curvature progression, possible chronic pain, psychological distress and possible reduced pulmonary function, early, and directed exercise prescription can facilitate long term health and productivity improvements in scoliosis patients. Hawes et al. also cites a need for more research on best practises after detailing historical problems with the approach of existing research (10).
Monticone et al. in 2014 conclude that rehabilitation programs including active self-corrections that focus on task orientated corrections and exercise as well as patient education have efficacy in reducing progression of spinal deformity and increasing health-related quality of life. It is however important to note that their observations were followed up for one year after which the intervention ended (1).
Kuru et al. in 2015 showed better results for Scroth method to a control group which was administered self-exercise at home. The Scroth group reported a lower Cobb angle, and the results of the other groups worsened. Patients were assessed pre-intervention at weeks 6, 12 and 24. (11)
Otman et. al in 2005, showed similar results with similar principle treatment protocols utilising the 3-Dimensional Scroth method for idiopathic scoliosis. Results recorded again at 6-weeks; 6-months; and 1-year showed a decrease in the Cob angle, however there was not a control group in this study.
The evidence for short term decreases in the cobb angle for up to a year post follow up certainly exists within the literature, and self-correcting programs through coaching and input by practitioners do show often superior results to other exercise programs with up to a year follow up. This includes the Scroth method which has plenty of evidence for its short-term validity are reported by the authors.
However, when many of these studies are further reviewed, in methodology and study design as well as referring to a systematic review by Mordecai et. al. (2012), reviewing the studies on decreased Cobb angles it is found that, they identified very few randomised control trials in adolescent idiopathic scoliosis (AIS). Concluding that most of the literature that show strong efficacy of intervention is weakly designed and do not have adequate control groups. Of the 9 studies examined only a single study had observer blinding. The review also noted that 5 out of the 10 studies all had conflicting interest and were all affiliated to centres that endorse exercise therapy for AIS. Recruitment of patients, age, sex respiratory function and radiographic parameters like Risser sign and other standard measurement practises for AIS. In Conclusion the “unbiased literature review has revealed poor quality evidence, for use of exercise therapy in treatment of AIS.” It is important that studies are publish using well-designed randomised controlled studies to properly assess, the role of exercise, as well as the different modalities used for these interventions.
With regards to another systematic review performed by Katharina et al. evidence published was cross referenced from and utilised from several authors from the same systematic review. This was done under the Schroth Spinal Deformities Rehabilitation Center in Germany. As can be seen, an independent review is needed for efficacy of these findings and the use of exercise therapy directed specifically for the treatment of AIS (11).
An interesting study comparing Cobb angles and other symmetrical measurements found improvement in both SEAS (scientific exercises approach to scoliosis) and core stabilisation, were similar in measurement. But the Core stabilisation group outperformed the SEAS group in the pain management scale based on the scoliosis research society 22-questionairre.
The most effective exercise methods for AIS indeed remains controversial (12). Long term results still seem to support orthopaedic long term studies that are dealing with a long term problem on the efficacy of the progression of AIS that points that scoliosis specific intervention is lacking a complete long term solution.
Discussion
A landmark study which presents a good proposition is the SOSORT 2018 winner – Which performed a high value randomised control trial in 2019 by Scheiber et al. They report that even if the Cobb angle did not improve beyond the accepted threshold of 5 degrees. Schroth treatment patients had an improvement in ‘perceived improvement in back status.’ They suggest that this study shows that it is worth considering alternatives to the Cobb angle which may be more relevant to patients. This is a very important study as it begins to think outside the box of the AIS trap – but rather suggest that we go back to outcome-based physiotherapy rather than trying to just fight back the Cobb angle (13).
At face value it shows efficacy in moving towards the biopsychosocial model that the profession of physiotherapy as a whole has consistently been moving in the UK as people start understanding that outcomes are of importance, but also the psychology and the patients’ needs must come first. We are not treating scoliosis but rather improving quality of life. And that includes self-efficacy – ability, activities of daily living as well as performance that is not only patient specific, but athlete specific. And adolescent needs to experiment, engage in different activities, interests, healthy living, sport, exercise. All these endeavours have unique and individualised demands on an adolescent.
Scoliosis has its own natural progression, but how can we keep the quality of life and what the patient sees most important at centre stage. Without rigorous evidence on the exercise effect on scoliosis and the different methodologies and programs that tailor to the condition rather than the wholistic picture of the individual physiotherapists can indeed miss the bigger picture. Programs such as Schroth although by their very nature are individualistic and catered in aligning the unique curves of each patient through stabilization and self-correction as well as postural control, in the end are only a small picture of what the patient, or rather, individual may want to achieve. There is also a limit indeed based on clinical best practise exercise science, that you can not hypertrophy and progress stabilisation indefinitely. So, although programs like PSSE’s (Dobomed, FITS, Lyon, Schroth, SEAS and side shift) definitely have efficacy and merit, you are not able to build strength and postural control in active sports, focusing only on these methods. An adolescent, desires to live a full and active life-style and as such, we must address all the drivers required for the safe, and efficient participation of the desired sport, physical activity and engagement.
It is also important to also understand the nature of various sports, and activities. A tennis player for example on service engages ground traction from the leg, through the hip and transfers this load through the spine. There is a co-activation of lower trunk muscles in order to stabilise the lumber spine. Under this amount of force, in such a short period, the player needs more than just local stabilisers however, or small corrective alignment of spine. A player in his sport, will be engaging also global stabilisers to exert force. And these strong rotational forces cannot be controlled or mediated through scoliosis specific exercises alone.
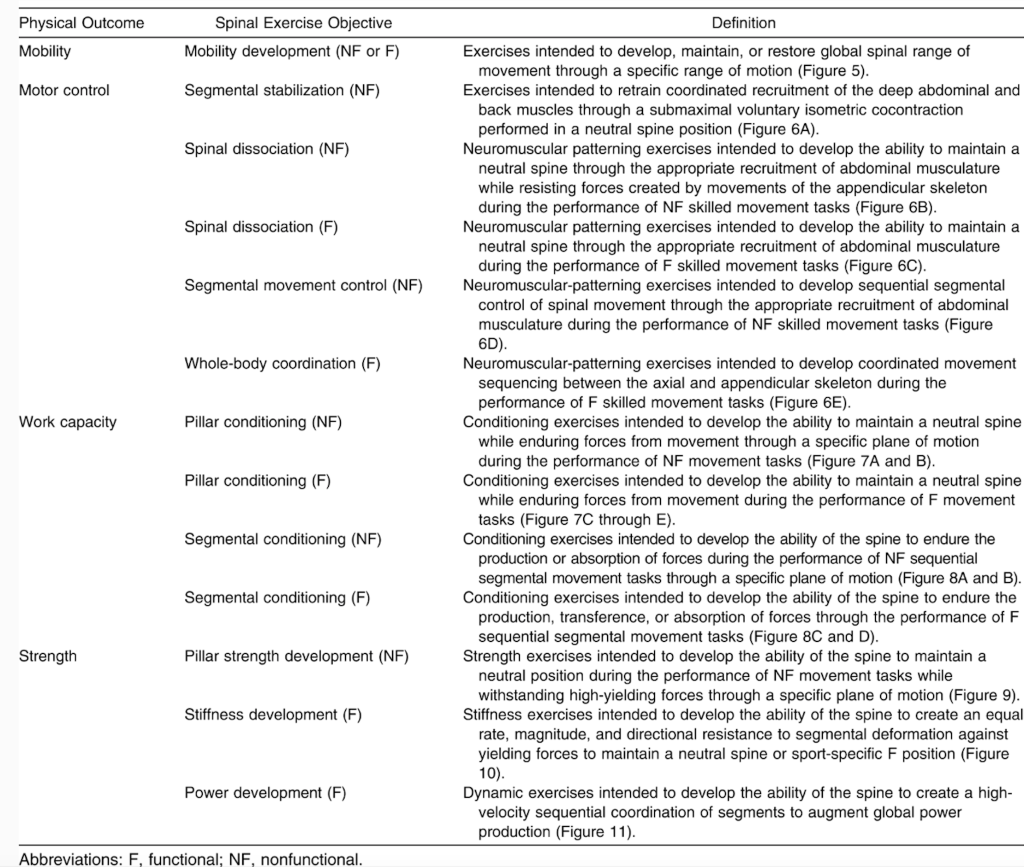
Indeed Mobility development, motor control, work capacity as well as strength must be developed for an athlete to not only compete safely in a sport but also in facilitating structural change and pillar strength if a therapist is even beginning of thinking of the possibility of improving postural control, and AIS in the long term. This however can not be thought of as AIS specific alone, but rather as holistic approach in order to create strength, and postural control in high torque motions that is required in any sport. This can be seen more completely in Figure. 1:
(Spencer, 2016 #279)
When addressing scoliosis with evidence-based practise, we need to have more considerations, as well as a holistic approach to what individual patient needs.
It’s important to familiarise ourselves with concepts such as “Give and Restriction” any long term plan for dealing with scoliosis as well as catering the adolescents needs with regards to efficient physical activity and healthy lifestyle.
“Give” is characterised as uncontrolled & excessive translation at a particular motion articular segment. It is an uncontrolled or excessive active ROM (Physiological) – Hypermobility/Instability. Characterised by a loss of motion or Restriction in the opposite direction. Site of pain is often termed the give, and the source the restriction. Treatment should focus on the restriction. This is where systems such as Schroth have shown to be of substantial use. Schroth, cannot really hypertrophy or change modular strength of intersegmental vertebrae, and this is likely why long-term results are scarce. It is a system that is built upon the ability for self-corrections in 3-dimesional space using breathing techniques, guided by a physiotherapist. There is however no evidence or reason to believe that this is a lifelong strategy of efficacy based on clinical reasoning, but rather a skill and tool, as well as stability exercise that allows the patient to be more cognisant of their posture, and learn how to make self-corrections, and become more independent in order to progress into periodisation and strength and conditioning, followed by sport specific considerations.
Possible identifiable postural dysfunctions that can be specifically and efficiently treated include:
Tight Hamstrings (Forcing thoracic ‘give’)
Tight Hip flexors (lordosis/kyphosis)
Leg length discrepancy can often lead to scoliosis.
Leg length discrepancy should be routinely checked as there is an abundance of evidence that something as simple as correcting leg length discrepancy with a podiatrist, fitting adequate lift has shown that it can help in correction of AIS and cobb angles. It is called after all ‘idiopathic’ scoliosis because we do not know the exact reason for why it happens. If we can determine an observable leg discrepancy, this is something that could be addressed. Leg length discrepancy can change as an adolescent child grows, therefore will need constant monitoring and possible adjustments. Raczkowski et al. reports that leg length discrepancy equalisation results in elimination of scoliosis (Raczkowski, 2010 #296).
Isolation of muscle groups has a lot of research how to best achieve this and which exercises can adequately isolate different muscle groups. There is no evidence for those who claim can isolate and consistently strengthen or hypertrophy interspinous or a specific area along the spinous process.
We do however have evidence on how to isolate, strengthen and hypertrophy various important muscle groups for trunk control.
Conclusion and final Considerations:
Short term efficacy of treatments based on a long term progressive disease with a plan limited that is effectively pure marketing is not really evidence based practise. Scroth and other marketed treatment concept for scoliosis are left lacking. Entire systems claiming superior methods for specific conditions is a tool of profiteering, not of evidence based practise.
The concepts, of stabilisation, postural control, as well as progression into hypertrophy, isolation work, multi-plane strength training, functional progression and sport specific exercise, with adaptations towards functional thriving in activities of daily living – incentivising exercise and quality of life, through a biopsychosocial model, where function supersedes physical image is of the utmost importance. Intelligent individualised exercise prescription is evidence based. General “marketed” “scoliosis” “specific “systems” simply are not. There is no evidence that any of these systems having significant results in disease progression long term. Therefore adapting exercise and specifically designing functional adolescent child scoliosis, protocols to allow them to best be able to engage in their most fulfilled functional lives is more important. And to do this, we can borrow from a plethora of information of evidence based literature, and should never be enclosed to “marketed systems” of “efficacy”. Sport specific is the answer to better lives.. After all – the fastest man on Earth – Ussain Bolt, has scoliosis. In order to run fast – one must be balanced, and strong. The simple ability of strengthening the body through movement, in physiological movement is more important than focusing on intersegmental stability for a life-time, which is an impossible goal. Proper positioning of the spine can-not be achieved through simple static exercise and breathing. Sure it forms a part, of an evidence based intervention, but can-not be the main focus.
References:
1. Monticone M, Ambrosini E, Cazzaniga D, Rocca B, Ferrante S. Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomised controlled trial. European Spine Journal. 2014;23(6):1204-14.
2. Negrini S, Bettany-Saltikov J, De Mauroy JC, Durmala J, Grivas TB, Knott P, et al. Letter to the Editor concerning: “Active self-correction and task-oriented exercises reduce spinal deformity and improve quality of life in subjects with mild adolescent idiopathic scoliosis. Results of a randomised controlled trial” by Monticone M, Ambrosini E, Cazzaniga D, Rocca B, Ferrante S (2014). Eur Spine J; DOI:10.1007/s00586-014-3241-y. European Spine Journal. 2014;23(10):2218-20.
3. Horne JP, Flannery R, Usman S. Adolescent idiopathic scoliosis: diagnosis and management. Am Fam Physician. 2014;89(3):193-8.
4. Tan KJ, Moe MM, Vaithinathan R, Wong HK. Curve progression in idiopathic scoliosis: follow-up study to skeletal maturity. Spine (Phila Pa 1976). 2009;34(7):697-700.
5. Greiner KA. Adolescent idiopathic scoliosis: radiologic decision-making. Am Fam Physician. 2002;65(9):1817-22.
6. Reamy BV, Slakey JB. Adolescent idiopathic scoliosis: review and current concepts. Am Fam Physician. 2001;64(1):111-6.
8. Płaszewski M, Bettany-Saltikov J. Are current scoliosis school screening recommendations evidence-based and up to date? A best evidence synthesis umbrella review. European Spine Journal. 2014;23(12):2572-85.
9. Lonstein JE. Natural history and school screening for scoliosis. Orthop Clin North Am. 1988;19(2):227-37.
10. Hawes MC. The use of exercises in the treatment of scoliosis: an evidence-based critical review of the literature. Pediatric Rehabilitation. 2003;6(3-4):171-82.
11. Mordecai SC, Dabke HV. Efficacy of exercise therapy for the treatment of adolescent idiopathic scoliosis: a review of the literature. European Spine Journal. 2012;21(3):382-9.
12. Yagci G, Yakut Y. Core stabilization exercises versus scoliosis-specific exercises in moderate idiopathic scoliosis treatment. Prosthet Orthot Int. 2019;43(3):301-8.
13. Schreiber S, Parent EC, Hill DL, Hedden DM, Moreau MJ, Southon SC. Patients with adolescent idiopathic scoliosis perceive positive improvements regardless of change in the Cobb angle – Results from a randomized controlled trial comparing a 6-month Schroth intervention added to standard care and standard care alone. SOSORT 2018 Award winner. BMC Musculoskeletal Disorders. 2019;20(1):319.
Author:
Constantinos Hadjichristofis – Bcom Human Resource Managment (Wits) PT (ACSM) BSc (Hons) Physiotherapy (Herts) MSc – Sports Medicine, Exercie and Health (UCL).
Regular exercise is arguably the most important thing that one can do for their health. Some of the immediate effects include the ability to control appetite, improve mode and sleep. Consistent exercise over a long period can help reduce heart disease, obesity, diabetes, depression, osteoarthritis, help improve autoimmune disorders, fibromyalgia, stroke as well as many cancers. In short, no condition or any form of healthy living is complete without exercise. Often when it comes to ones health, we look for different genesis of certain conditions as to why we are not feeling well. Movement and exercise however is absolutely a lifestyle adaptation necessary not only for peak health, but for maintenance of health.
Exercise Recommendation for Adults:
According to he American College of Sports Medicine (ACSM) adults should at a minimum be engaging in exercise for 150 minutes of moderate exercise or 75 minutes of vigorous exercise a week.
Strength exercise that works all major muscle groups is indicated. Strength training can involve the safety of isolation muscle specific exercise, or across multiple groups of muscles at once. There are many different approaches and evidence based prescription of exercise, but essentially, a program that involves gradual increase of resistance over time is necessary.
Pregnancy
Clementine Yogi -demonstrates some pelvic floor exercises for Pregnancy.
Aerobic Exercise is safe for pregnant women. 30 minutes of walking a day is indicated. Pelvic floor strengthening, stomach strengthening exercises, pelvic tilt exercises are all indicated.
Avoid lying flat on your back for long periods (particularly after 16 weeks), to avoid blocking blood flow back to your heart, that can make you feel faint.
It is important in this period however to avoid contact sports, such as kickboxing, judo.
Altitude sickness is something the baby has no protection against. Therefore scuba-diving and climbing at altitude (over 2,500m is contra-indicated.)
Children
Children, according to the ACSM should engage in physical activity for at least 60 minutes every single day. Mostly this is geared towards aerobic exercise. Strength training and vigorous exercise, should also be done at least 3 times a week.
Ultrasound, laser and magnetic therapy, is often frequently used by many Physical therapists with the reasoning of reducing pain and improve rehabilitation outcomes. The problem however is that properly conducted studies are categorically showing that it makes no difference at all, and it is wasted time from your session. Indeed, if your physical therapist is using all of these modalities and rotating the patient from machine to machine, the efficacy of the treatment is about as good as throwing your money down the drain.
Physical Therapists need to follow evidence-based care. Physiotherapists are now allied health care professionals. The profession is somewhat a newer entry into a respected health care professional, and as physiotherapists are producing their own research in the best modalities for treating musculoskeletal conditions, the era of “Guru’s” as well as companies driving sales on inefficient machines must come to an end. It is absolutely criminal at this stage to sell patients this type of snake oil interventions, when the research absolutely does not support their use. Its time for a new generation of Physical Therapists to bring back the evidence into physical therapy. The good news is that new graduates are now aware of the importance of exercise, as a primary driver of rehabilitation, but we also need to address the lingering effects of a profession that all too often is guided by dinosaurs, and for-profit marketeers of non-scientific machines.
Ultrasound:
There is now a plethora of research and systematic reviews showing ultrasound to be non-evidence-based practise with no benefit.
musculoskeletal disorders
strongly negative review of 13 “adequate” trials did not support “the existence” of therapeutic effects (van der Windt, 1999 #372)
pain and injury
“little evidence” of therapeutic benefit in 10 “acceptable” trials out of 35 candidates; 2 positive trials, 8 negative (Robertson, 2001 #373)
biological effects
“insufficient biophysical evidence” to justify therapeutic use for pain and injury (Baker, 2001 #374)
tennis elbow
nine studies produced “platinum” level (better than gold!) evidence of “little or no benefit” (for ESWT)(Buchbinder, 2006 #375)
tennis elbow
conflicting, “unconvincing” evidence of efficacy from a few trials (of ESWT again) (Ho, 2007 #376)
rotator cuff tendinopathy
limited evidence “supports … ESWT for chronic calcific rotator cuff tendinitis,” but no non non-calcific (Ho, 2007)
osteoarthritis of knee
a positive update to a previously negative review, which is strange because it’s based on just 5 small, poor quality trials with trivial “positive” results (Rutjes, 2010 #378)
lower limb conditions
inconclusive review of 10 of 15 candidates: “no high quality evidence available” (Shanks, 2010 #379)
ankle sprains
inconclusive but discouraging review of “five small placebo-controlled trials”; the “potential treatment effects of ultrasound appear to be generally small” (van den Bekerom, 2011 #380)
carpal tunnel syndrome
inconclusive but slightly encouraging review of “only poor quality evidence from very limited data” from 11 trials (Page, 2013 #381)
chronic low back pain
inconclusive and underwhelming review of 7 small trials, none of them good quality (Ebadi, 2014 #382)
rotator cuff tendinopathy
negative review “does not provide any benefit … based on low to moderate level evidence” from 11 weak trials(Desmeules, 2015 #383)
(Ingraham, 2018)
HO, C. 2007. Extracorporeal shock wave treatment for chronic rotator cuff tendonitis (shoulder pain). Issues Emerg Health Technol, 1-4.
“An 18-year-old England women’s football player tears her ACL 12 weeks prior to the Olympic Games. She is a key player and has been through 4 years of training in preparation and wants to compete. It is an isolated complete ACL tear with no other knee structures damaged. She decides to rehabilitate conservatively rather than having surgery in order to prepare and not miss the games.”
Table of Contents:
Introduction
Biomechanics of Football – Predisposing ACL Risk Factors in Women
Predisposing ACL Risk Factors in Women
Intrinsic Factors
Extrinsic Factors
Goals for Rehabilitation
Assessment
Early: Acute Phase of Rehabilitation:
Middle: Neuromuscular Phase
Late: Return to Sport Phase
Return to Sport Assessment
Introduction:
The Olympic Games are a Pinnacle in athletic sporting achievement. In this Essay, we will highlight biomechanics that need to be achieved and avert risk to the Athlete. Predisposing risk factors of the injury and how they will be addressed. Goals of rehabilitation during the 12-week rehabilitation course in the different stages. Strategies and interventions utilised. And a criteria-based evaluation, on when it is appropriate to proceed to the next stage of rehabilitation, return to training, and then to the sport, and competitive play.
Biomechanics of Football – Predisposing ACL Risk Factors in Women
Football consists of a wide range of Skills, that can invariably put the ACL at risk. First it is apt to define the common injury mechanism of the ACL. Direct Contact is seen in 30% of cases. (1) Non-Contact is characterised by 70% of cases (1) in all ACL injuries, and this is predominantly the group associated with football ACL injury. The group that rehabilitation and intervention have the most effect in preventing a re-injury is indeed the non-contact group as neuromuscular control, strength and conditioning play a significant role in prevention of such injuries. (2) Female athletes have a four to six times larger incidence in ACL injury in sports that require cutting and jumping. (3) In women football players it was found to be correlated with more joint laxity and hyperextension in the joints. (4) Joint Hyperextension was found to increase incidence of ACL Injury. (5) Indeed the mechanism for ACL injury, usually involves a “cut and plant” movement, with the leg firmly planted into ground with a vulgus force. Deceleration, and changes in direction are all mechanisms of injury, and prevalent in the biomechanics of football. (6) Walden et al. show that the three most prevalent mechanisms in non-contact ACL injury, involve, “pressing”, “re-gaining balance after kicking” and “landing after a header”. (7) All these situations, often involve unexpected perturbations of balance and sudden landing or unexpected change of direction with the knee hyperextension, or slightly bent in a vulgus rotational force position. (7)
Predisposing ACL Risk Factors in Women
Intrinsic Factors
Stability of the knee is influenced by structural integrity, together with mechanical alignment in movement. Certain intrinsic factors are inherent and non-modifiable. Women have a different pelvic width as well as tibiofemoral angle, to men. (8) A larger Q-Angle in women (9) (Figure- 1) combined with the femoral notch width are considered as significant anatomical factors that predispose women to higher incidence of ACL injury. (10) In theory, a greater Q-Angle predisposes an individual to greater lateral pull of the quadriceps-femoris muscle to the patella causing knee tension medially. Highlighting importance of Quad and hamstring strength.(11)
Figure-1: Static Q Angle
(10)
Hormonal influence in women is also gaining increasing support in the literature for ACL injury as a risk factor with greatest risk of injury identified 1 or 2 days after onset of menses. This information can be used to be more careful with the athlete during that time. (12)
Relative deficits in neuromuscular control, Strength of muscle (13), postural alignment and control (14) as well as landing characteristics (15) also show increased risk in women compared to men. However, they are also regarded as predominantly modifiable. (16) Efficient strength and conditioning programs, and athletic specific training showsignificant promise in influencing possible deficits. (17) Knee stiffness is also considered a significant conjunct to knee stability as well as injury prevention. Mechanoreceptors can modulate joint ligamentous and muscle laxity stiffness. (18)
Extrinsic Risk Factors
There are several factors of extrinsic risk, many are non-modifiable, however important to consider, to safely return the athlete to sport. Things like surface and shoe type, pitch type. Working from hard steady ground with athletic trainers, to grass pitch, and the use of football cleats. Lambson at al. (1996) show that football cleats increase traction substantially, and this has a corelative effect with increased incidence of ACL injury. (19) Other factors include, the general fitness level of elite Olympic women’s football players. Our patient, must be ready to play in 12 weeks, and as such must maintain a fitness level that would not put her at increased risk of injury, but also be able to maintain and perform at the required cardiovascular strength and speed, of the game she is being prepared for, and therefore must maintain her fitness pre-injury and build on it. (20) (21) These factors must all be considered, into the return to sport training phase.
Goals for Rehabilitation
Focus should be targeted towards modifiable intervention, which will focus primarily on prevention of non-contact (loosely defined as non-direct outside force to knee structure) as well as catered specifically for the demands and level of the sport and level of play (elite women’s football – Olympics). A Physiological and Psychological assessment should be conducted for return to play, and to manage expectations and motivation throughout the process, as only a small percentage of players will be able to return to pivoting and cutting sports without knee-reconstruction. (22)
Assessment
Conservative ACL Rehab treatment can be considered since there are no other concomitant injury. In order for non-operative treatment of ACL rehabilitation to return to cutting and pivoting sports, it is necessary to identify “Potential coppers”. This is done through a number of screening tests. (23) As seen in Table-1
Table 1: Screening tests of “Coppers vs Non-Coppers” suitable for ACL non-operative
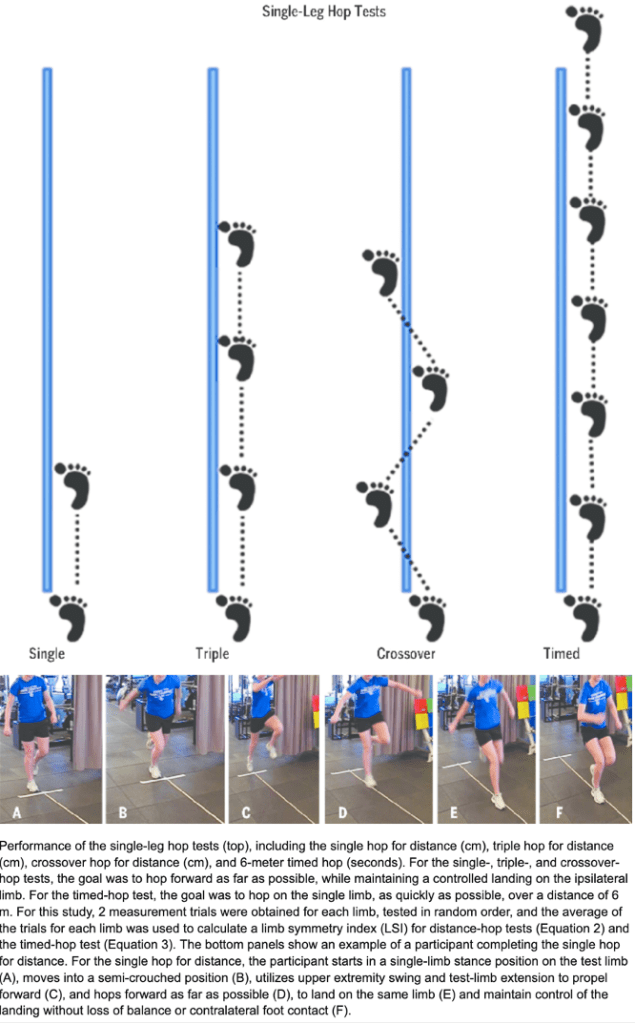
Hop testing. (One legged distance, triple hop, cross over hp and 6m timed hop test).
Minimum of 80% limb symmetry
Knee giving way report
1 Subjective report
Self-reported global knee function rating.
>60
Knee Outcome survey/Activity of Daily Living scale
>80%
(23)
The screening tests are vital if the patient wants to return to Cutting/pivoting sport. If they cannot meet it is more likely they will have to reduce physical activity and be classified as a ‘Non-copper’. (24) Our patient has been identified as a Copper.
Figure-2: Hop-Testing
(25)
Early: Acute Phase of Rehabilitation:
Homeostasis; ROM Muscle Activation: Focus on restoration of joint homeostasis and Active Range of motion (ROM). Hemarthrosis must be reduced. Cryotherapy and compression help in an aggressive approach to manage acute effusion. (26)
Goals:
Activation: Improve integrity of motion and muscle activation. Utilisation of wall slides as well as stationary bike. Can start also with quadricep isometric contraction. (10) Facilitation of Patellofemoral glide through manual therapy and activation of Quadriceps, and NMES (27) in medio-cephalic direction is desirable (28) (29).
Strength: A focus on quadriceps should utilise open chain exercise (OKC) and closed kinetic chain (CKC) should be utilised together as tolerated as OKC targets isolated quadriceps whilst CKC has more dynamic application. OKC limited to 30-100 flexion to reduce “anterior shearing” in knee. (30)
Strength training in acute phase should also address any identified weakness in hamstring, hip and core. (31) Any deficits in trunk control are a significant risk to re-injury and should be addressed. (32)
Middle: Neuromuscular Phase
Progression Indicators: Effusion controlled, Achieved full ROM, Base lower extremity strength allowing for participation in more dynamic weight bearing exercise. (32)
Goals: Continued focus on lower extremity strength, with addition of neuromuscular training, balance, proprioception, stability, continue strength building, and move into power as well as maintain and build Cardio-vascular requirements, for football. (32) Elite athletes must maintain, and progress fitness and strength in non-injured sites.
Perturbation Exercise: Literature shows significant efficacy of putting patients on surfaces challenging their balance state, and unexpected perturbations utilised to challenge their ability to maintain balance. (33)
Figure 3: Perturbation Training
(34)
Late: Return to Sport Phase
Progression Indicators: No Episodes of “giving way” during neuromuscular phase. Hamstring and Quadricep strength must have advanced and demonstrated through isometric testing as 90% of contra-lateral limb. (32)
Goals: Return to play to cutting and pivoting must be geared to sport specific integration of sport. This must be done systematically and gradually. There is evidence that a brace, can help in accommodating this transition and accommodating patient stability reducing anterior tibial translation and proprioceptive feedback. (35)
Figure-4: Cutting and Pivoting Drill for 6 weeks Resulted in Meaningful results in youth Soccer Players. (35)
(36)
Stages: Continue with straight line running at non-maximal speed, that is slowly progressed to changes in direction and running in various planes of movement eventually progressing to full speed changes of direction (37), and then integrated to sport specific movements, ball control, kicking the ball. Finally progress to injury vulnerable states of loading, to facilitate a safe return and avoid re-injury. (38) Cardiovascular and strength training and requirements of activity must be simultaneously maintained, as the athlete must return to elite level sport, and is expected to meet the cardiorespiratory and fitness requirements. (32)
Return to Sport Assessment
Return to sport testing and assessment should be conducted through an objective analysis of lower limb strength, functional kinematics as well as ability to integrate to specific demands of the sport. Physiological (39) and psychological readiness also play a significant role. (32) Isokinetic strength of Quadriceps and hamstrings, as well as hop tests described in initial assessment should have >90% co-symmetry. (40) (41).
Tuck Jump and single leg squat assessments can be used to test asymmetries. (42)
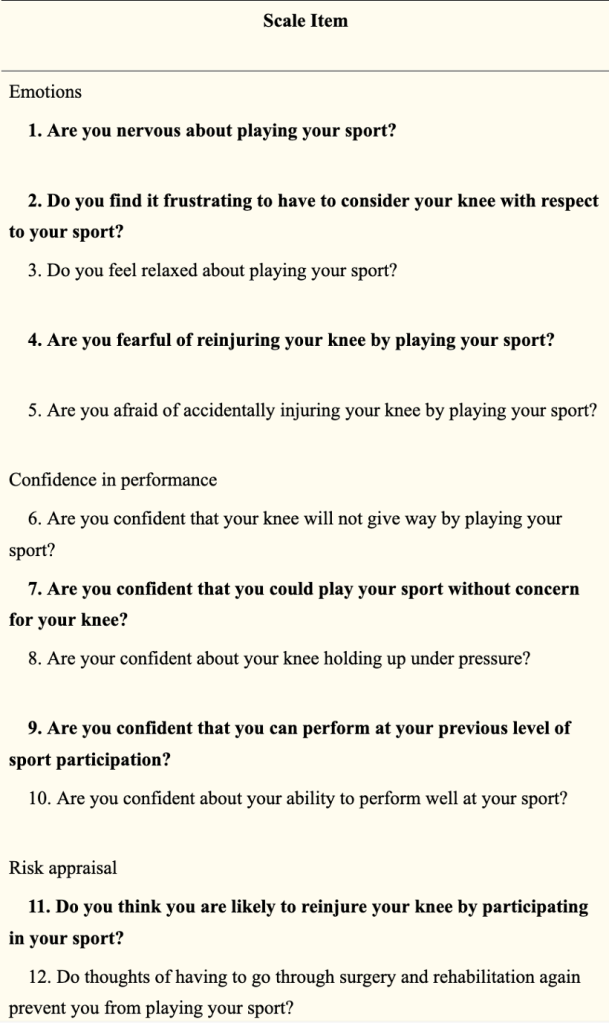
For the Psychological component we can use the “12-Item ACL-Return to Sport (ACL-RSI) scale”. (39)
Sport Specific readiness assessed through systematic increases of load and subjective monitoring, of sport specific functions movement, and fitness levels.
Figure-5: (ACL-RSI) scale
Conclusion
The goal is to return the player safely to her sport, by considering all the risk factors, both intrinsic and extrinsic and working towards strength, neuromuscular control, inherent dynamics of football which is a cutting and pivoting sport. The athlete must be able to take on all the demands the sport can put them under, with increased loads and eventual stressing of knee towards loads and positions that could be considered injury vulnerable states. The physiotherapist must be happy with the athlete’s progression at every stage before giving the clear and go ahead to progress, objectively as well as subjectively, and utilize a diagnostic approach. (43) The athlete can-not progress without reaching each goal set for him, even if time is constrained. One vital aspect not often considered is the athletes psychological state, after the rehabilitation is completed. (32) The athlete must also have confidence in the work put in, therefore the athletes psychological state in itself should be the final barrier to overcome once the therapist is happy with achievement of his physiological sport-specific objectives.
References:
1. McNair PJ, Marshall RN, Matheson JA. Important features associated with acute anterior cruciate ligament injury. N Z Med J. 1990;103(901):537-9.
2. Dhillon H, Dhillon S, Dhillon MS. Current Concepts in Sports Injury Rehabilitation. Indian J Orthop. 2017;51(5):529-36.
3. Hewett TE, Myer GD, Ford KR. Anterior Cruciate Ligament Injuries in Female Athletes. The American Journal of Sports Medicine. 2006;34(2):299-311.
4. Wojtys EM, Huston LJ, Lindenfeld TN, Hewett TE, Greenfield MLV. Association between the menstrual cycle and anterior cruciate ligament injuries in female athletes. The American journal of sports medicine. 1998;26(5):614-9.
5. Hewett TE, Myer GD, Ford KR, Paterno MV, Quatman CE. Mechanisms, prediction, and prevention of ACL injuries: Cut risk with three sharpened and validated tools. Journal of Orthopaedic Research. 2016;34(11):1843-55.
6. Pfeifer CE, Beattie PF, Sacko RS, Hand A. RISK FACTORS ASSOCIATED WITH NON-CONTACT ANTERIOR CRUCIATE LIGAMENT INJURY: A SYSTEMATIC REVIEW. Int J Sports Phys Ther. 2018;13(4):575-87.
7. Waldén M, Krosshaug T, Bjørneboe J, Andersen TE, Faul O, Hägglund M. Three distinct mechanisms predominate in non-contact anterior cruciate ligament injuries in male professional football players: a systematic video analysis of 39 cases. British Journal of Sports Medicine. 2015;49(22):1452-60.
8. HUNGERFORD DS, BARRY M. Biomechanics of the Patellofemoral Joint. Clinical Orthopaedics and Related Research®. 1979(144):9-15.
9. Hahn T, Foldspang A. The Q angle and sport. Scand J Med Sci Sports. 1997;7(1):43-8.
10. Huston LJ, Greenfield MLVH, Wojtys EM. Anterior Cruciate Ligament Injuries in the Female Athlete: Potential Risk Factors. Clinical Orthopaedics and Related Research®. 2000;372:50-63.
11. SHAMBAUGH JP, KLEIN A, HERBERT JH. Structural measures as predictors of injury in basketball players. Medicine & Science in Sports & Exercise. 1991;23(5):522-7.
12. Slauterbeck JR, Fuzie SF, Smith MP, Clark RJ, Xu K, Starch DW, et al. The Menstrual Cycle, Sex Hormones, and Anterior Cruciate Ligament Injury. J Athl Train. 2002;37(3):275-8.
13. Griffin JW, Tooms RE, vander Zwaag R, Bertorini TE, O’Toole ML. Eccentric muscle performance of elbow and knee muscle groups in untrained men and women. Med Sci Sports Exerc. 1993;25(8):936-44.
14. Huston LJ, Wojtys EM. Neuromuscular performance characteristics in elite female athletes. Am J Sports Med. 1996;24(4):427-36.
15. Colby S, Francisco A, Yu B, Kirkendall D, Finch M, Garrett W, Jr. Electromyographic and kinematic analysis of cutting maneuvers. Implications for anterior cruciate ligament injury. Am J Sports Med. 2000;28(2):234-40.
16. Caraffa A, Cerulli G, Projetti M, Aisa G, Rizzo A. Prevention of anterior cruciate ligament injuries in soccer. A prospective controlled study of proprioceptive training. Knee Surg Sports Traumatol Arthrosc. 1996;4(1):19-21.
17. Hewett TE, Stroupe AL, Nance TA, Noyes FR. Plyometric training in female athletes. Decreased impact forces and increased hamstring torques. Am J Sports Med. 1996;24(6):765-73.
18. Sojka P, Sjolander P, Johansson H, Djupsjobacka M. Influence from stretch-sensitive receptors in the collateral ligaments of the knee joint on the gamma-muscle-spindle systems of flexor and extensor muscles. Neurosci Res. 1991;11(1):55-62.
19. Lambson RB, Barnhill BS, Higgins RW. Football cleat design and its effect on anterior cruciate ligament injuries: a three-year prospective study. The American journal of sports medicine. 1996;24(2):155-9.
20. Njororai Simiyu W. Physical demands of soccer: Lessons from team USA and Ghana matches in the 2010 FIFA WORLD CUP. Journal of Physical Education and Sport. 2012;12:407-12.
21. Ingebrigtsen J, Dillern T, Shalfawi SA. Aerobic Capacities and Anthropometric Characteristics of Elite Female Soccer Players. The Journal of Strength & Conditioning Research. 2011;25(12):3352-7.
22. Fabricant PD, Lakomkin N, Cruz AI, Spitzer E, Marx RG. ACL reconstruction in youth athletes results in an improved rate of return to athletic activity when compared with non-operative treatment: a systematic review of the literature. 2016;1(2):62-9.
23. Soltani N, Rahimi A, Naimi S-S, Khademi K, Saeedi H. Studying the Balance of the Coper and Non-Coper ACL-Deficient Knee Subjects. Asian J Sports Med. 2014;5(2):91-8.
24. Hurd WJ, Axe MJ, Snyder-Mackler L. A 10-year prospective trial of a patient management algorithm and screening examination for highly active individuals with anterior cruciate ligament injury: Part 2, determinants of dynamic knee stability. The American journal of sports medicine. 2008;36(1):48-56.
25. Schmitt L, Paterno M, Hewett T. The Impact of Quadriceps Femoris Strength Asymmetry on Functional Performance at Return to Sport Following Anterior Cruciate Ligament Reconstruction. The Journal of orthopaedic and sports physical therapy. 2012;42:750-9.
26. Hurd W, Axe M, Snyder-Mackler L. Management of the athlete with acute anterior cruciate ligament deficiency. Sports Health. 2009;1(1):39-46.
27. Snyder-Mackler L, Ladin Z, Schepsis AA, Young J. Electrical stimulation of the thigh muscles after reconstruction of the anterior cruciate ligament. Effects of electrically elicited contraction of the quadriceps femoris and hamstring muscles on gait and on strength of the thigh muscles. The Journal of bone and joint surgery American volume. 1991;73(7):1025-36.
28. Suter E, McMorland G, Herzog W, Bray R. Conservative lower back treatment reduces inhibition in knee-extensor muscles: a randomized controlled trial. Journal of Manipulative and Physiological Therapeutics. 2000;23(2):76-80.
29. Bousquet B, O’Brien L, Singleton S, Beggs M. POST-OPERATIVE CRITERION BASED REHABILITATION OF ACL REPAIRS: A CLINICAL COMMENTARY. Int J Sports Phys Ther. 2018;13.
30. Beynnon BD, Fleming BC, Johnson RJ, Nichols CE, Renström PA, Pope MH. Anterior cruciate ligament strain behavior during rehabilitation exercises in vivo. The American Journal of Sports Medicine. 1995;23(1):24-34.
31. Hewett TE, Torg JS, Boden BP. Video analysis of trunk and knee motion during non-contact anterior cruciate ligament injury in female athletes: lateral trunk and knee abduction motion are combined components of the injury mechanism. British journal of sports medicine. 2009;43(6):417-22.
32. Paterno MV. Non-operative Care of the Patient with an ACL-Deficient Knee. Curr Rev Musculoskelet Med. 2017;10(3):322-7.
33. Chmielewski TL, Rudolph KS, Snyder-Mackler L. Development of dynamic knee stability after acute ACL injury. Journal of Electromyography and Kinesiology. 2002;12(4):267-74.
34. Hurd WJ, Chmielewski TL, Snyder-Mackler L. Perturbation-enhanced neuromuscular training alters muscle activity in female athletes. Knee Surgery, Sports Traumatology, Arthroscopy. 2006;14(1):60-9.
35. Beynnon BD, Fleming BC, Churchill DL, Brown D. The effect of anterior cruciate ligament deficiency and functional bracing on translation of the tibia relative to the femur during nonweightbearing and weightbearing. The American journal of sports medicine. 2003;31(1):99-105.
36. Dos’Santos T, McBurnie A, Comfort P, Jones PA. The Effects of Six-Weeks Change of Direction Speed and Technique Modification Training on Cutting Performance and Movement Quality in Male Youth Soccer Players. Sports. 2019;7(9):205.
37. Fitzgerald GK, Axe MJ, Snyder-Mackler L. Proposed practice guidelines for nonoperative anterior cruciate ligament rehabilitation of physically active individuals. Journal of Orthopaedic & Sports Physical Therapy. 2000;30(4):194-203.
38. Blanch P, Gabbett TJ. Has the athlete trained enough to return to play safely? The acute: chronic workload ratio permits clinicians to quantify a player’s risk of subsequent injury. Br J Sports Med. 2016;50(8):471-5.
39. Webster KE, Feller JA, Lambros C. Development and preliminary validation of a scale to measure the psychological impact of returning to sport following anterior cruciate ligament reconstruction surgery. Physical therapy in sport. 2008;9(1):9-15.
40. Ithurburn M, Paterno M, Ford K, Hewett T, Schmitt L. QUADRICEPS FEMORIS STRENGTH ASYMMETRY DIFFERENTIATES SINGLE-LEG DROP-LANDING MECHANICS AT RETURN TO SPORT IN YOUNG ATHLETES AFTER ANTERIOR CRUCIATE LIGAMENT RECONSTRUCTION: SPL34. journal of Orthopaedic & Sports Physical. 2015;45(1).
41. Nagai T, Schilaty ND, Laskowski ER, Hewett TE. Hop tests can result in higher limb symmetry index values than isokinetic strength and leg press tests in patients following ACL reconstruction. Knee Surgery, Sports Traumatology, Arthroscopy. 2020;28(3):816-22.
42. Myer GD, Ford KR, Hewett TE. Tuck jump assessment for reducing anterior cruciate ligament injury risk. Athletic therapy today: the journal for sports health care professionals. 2008;13(5):39.
43. Weiler R, Monte-Colombo M, Mitchell A, Haddad F. Non-operative management of a complete anterior cruciate ligament injury in an English Premier League football player with return to play in less than 8 weeks: applying common sense in the absence of evidence. BMJ Case Reports. 2015;2015:bcr2014208012.
Exercise Program:
Acute Phase:
Rehabilitation must be outcome based. And cannot proceed without goals and progression indicators being met.
The following is a retrospective Hypothetical Progression Scenario.
Week 1-4
Relative rest, elevation, cryotherapy to Reduce swelling and inflammation.
Activation: Improve integrity of motion and muscle activation. Utilisation of wall slides as well as stationary bike. Can start also with quadricep isometric contraction. (10) Facilitation of Patellofemoral glide through manual therapy and activation of Quadriceps, and NMES (27) in medio-cephalic direction is desirable (28) (29).
Strength: A focus on quadriceps should utilise open chain exercise (OKC) and closed kinetic chain (CKC) should be utilised together as tolerated as OKC targets isolated quadriceps whilst CKC has more dynamic application. OKC limited to 30-100 flexion to reduce “anterior shearing” in knee. (30)
Active-Assisted Extension, Using opposite leg to straighten quadriceps 90 – 0 degrees Avoid hyperextension
5 times, 30 second hold end range.
Increase Range of Motion
Wall slides, PROM Lie on back injured leg on wall
Slowly slide leg down Hold max flexed position 30 seconds – Repeat 5 times
Quadricep Activation
Activation of quad (VMO) Gain Extension ROM Upwards and mediaal activation and hold Isometric Hold
!0-15 Reps !0 Second hold 3 Sets
Gain ROM – Flexion
Leg Slides on bed.
Pull heel towards buttocks
Week 2:
Week 2
Goals
Monday-Sunday Exercise
exercise
Repetitions/Once Daily Unless otherwise Indicated
Continue Week 1 Exercises
Week 1 Exercises
Week 1 Exercises
Week 1 exercises
100 Degree Flexion Achieved ROM Increase Strength Minimal resistance
Cycling
20 Mins Twice daily
Straigh leg raise Strength quad
SLR – Side to Side – down
3 Sets 15 Repetions
Glute Strength Core Strength
Hip Extension/Bridge
3 sets 15 Repetions
Hip Abd/Add/
Hip Abd/Add
3 sets 15 Repetions
Quad Strength Glute strength Partial range
Body Weigh Squats
2-3 Sets 10-20 Repetitions
Quad Strength Hamstring eccentiric
Standing TKE with Theraband/cable
3 Sets 15 Repetions
Hamstring Stength
Standing or prone hamstring curls
3 Sets of 15 Repetitions
Gastroc Strengthening
Heel raises
3 Sets of 15 Repetitions
Start low impact, cardio, sport Specific.
Anti-gravity Run (70% body weight, progressed to 80 then 90)
30 mins Once a day 5x per week Start at walk work to jog
Wekk 3-4
Week 3-4
Goals: Progression
Monday-Sunday Exercise
exercise
Perform Strengthening Exerices 3-5 Times a week.
100 Degree Flexion Achieved ROM Increase Strength Minimal resistance
Cycling
20 Mins Once a day 5x per week
Improme ROM/Flexibility
“Continue ROM/Flexibility Exercises “
Week 1 Exercises
Work on ROM as per week 1
Continue Open Chain/Progress with increased weight.
Hip/Knee Exercises
Week 2 Exercises
Week 2 exercises
Quad & Hamstring strength Exercise Progression
Hamstring Curl Machine Quadricep Machine
3 Sets 12 rep 70%!RM – 3x week
Leg Press
Leg Press (Progress double-Single leg)
3 sets 12 reps 3x per week 70% !RM
Quad glute Strengthening/ Stability
Hamstring strength Exercise Progression (foreward and lateral)
3 sets 15 reps 3x per week
Glutes Quads, Stability, Core
Squat 90 degrees
3 Sets 12 reps 80%1RM3x per week
Core stability
Plank/Side-plank
2 Sets 30 seconds 5x per week
Gluts, core stability control hip extensor.
Single Limb Bridge
2 Sets 15 seconds 5x per week
Begin Proprioception Training Progress to eyes closed
Bosu half Ball
30-60 seconds 5 times per week
Start low impact, cardio, sport Specific.
Anti-gravity Run (70% body weight, progressed to 80 then 90)
20 mins Once a day 5x per week Start at low Impact
Middle: Neuromuscular Phase
Progression Indicators: Effusion controlled, Achieved full ROM, Base lower extremity strength allowing for participation in more dynamic weight bearing exercise. (32)
Goals: Continued focus on lower extremity strength, with addition of neuromuscular training, balance, proprioception, stability, continue strength building, and move into power as well as maintain and build Cardio-vascular requirements, for football. (32) Elite athletes must maintain, and progress fitness and strength in non-injured sites.
Perturbation Exercise: Literature shows significant efficacy of putting patients on surfaces challenging their balance state, and unexpected perturbations utilised to challenge their ability to maintain balance. (33)
Monday
Lower body strength & cardio
Tuseday
Lower body (week 4-6)/Plyometrics (week 6-8) & upper body strength
Deltoid, Trapezius, Serratus and terior Core stabilisation
Military Press
Sets: 2 Reps 12-15 80%1RM Rest 60 Seconds
Warm Down
1500m Light jog Light static stretch Recovery
Hamstring/Quad/add stretch Stretch for recovery as needed.
Core Stability – Perturbation
Week 4-8
Goals: Progression
Stability – Perturbation
exercise
Sets/Reps
Increase HR
Warm- up – Cycling
15 mins
Functional dynamic activation
3- step Hold stabilise Backwards and foreward High Knee skips Back Pedals Lateral Lunge walks Single leg alternating holds Single leg lift
Functional Movements, 20m Each
Achieve balance, stability Advance with ball throw
Single leg Bosu exercise Balance.
30 second x 10 reps
Rectus abdominus; Stability Functional, Core.
Sit ups with medicine ball throw
Reps 15 Sets 3.
Core stability, Hip flexors, Eccentric load contro With Press up.l
TRX Forward facing full body Flexion.
Reps 15 Sets 3
Functional/dynamic Stability
Pertubation: Box up with Directional offbalance.
Reps 15 Sets 2
Stability balance SL Pertubation
Single leg hold squat.
Hold 30 seconds – 5 times, Each leg
Stability Control
Side Plank
30 second x 3 reps
Stability Control
Front Plank
30 seconds x 3 reps
Stability, and movement, all 4 limbs
All 4’s Hold follow ball
30 seconds x 3 reps
Neuromusclular control, and fulll body core, and stability
Bosu ball front facing Crunch
15 Reps 3 sets
Warm down
Warm Down – slow cycle Passive stretch/Foam roller
10 mins
Late: Return to Sport Phase Week 8-11
Progression Indicators: No Episodes of “giving way” during neuromuscular phase. Hamstring and Quadricep strength must have advanced and demonstrated through isometric testing as 90% of contra-lateral limb. (32)
Progress to power, when athlete is able to Run/jog on Anti-Gravity treadmill at least 90 percent Gravity; Squat 80% of 80% of 10 RM, Leg at 4cm dif of Y-test. Hamstring Quad ration at 60% on dynamometer. (32)
Goals: Return to play to cutting and pivoting must be geared to sport specific integration of sport. This must be done systematically and gradually. There is evidence that a brace, can help in accommodating this transition and accommodating patient stability reducing anterior tibial translation and proprioceptive feedback. (35)
Stages: Continue with straight line running at non-maximal speed, that is slowly progressed to changes in direction and running in various planes of movement eventually progressing to full speed changes of direction (37), and then integrated to sport specific movements, ball control, kicking the ball. Finally progress to injury vulnerable states of loading, to facilitate a safe return and avoid re-injury. (38) Cardiovascular and strength training and requirements of activity must be simultaneously maintained, as the athlete must return to elite level sport, and is expected to meet the cardiorespiratory and fitness requirements. (32)
Monday
Lower body Power & Sport Specific Cardio
Tuseday
Plyometrics & upper body strength
Wednesday
Low load recovery (Sport Specific-Perturbation-Stability) & Sport Specific cardio
Thursday
Same as Monday
Friday
Same as Tuseday
Saturday
Same as Wednesday
Sunday
Off
Lower Body Power
Week 8-11
Middle: Neuromuscular Phase
Exercise – Lower Body Power
exercise
Neuromuscular & Strength
100 Degree Flexion Achieved ROM Increase Strength Minimal resistance
Cycling
20 Mins
Glutes Quads, Stability, Core
Squat 90 degrees
3 Sets 4-6 reps 80%1RM Progression: Build power Drop reps to 6; Increase load
Quad glute Strengthening/ Stability
Lunges with Weight
3 sets 4-6 reps 90% 1RM
Hamstring Isolation
Nordics
2 sets 5 Reps Progress Reps Sets over time.
Quad Isolation
Quadricep Machine
3 sets 4-6 Reps 80% 1 RM
Build Quad, and Glute strength Slow eccentric down
Work On Change of direction Technique, and explosive change of direction
Cut and Plant, Cone runs Quick steps
20 repetitions
Greater Power progression
Ice Skaters Side to side Jump and hold
15 reps/3 sets
Warm Down
1500m Light jog Light static stretch Recovery
Hamstring/Quad/add stretch Stretch for recovery as needed.
Sport Specific – Conditioning:
Week 8-11
Late: RTP
Exercise – Field Training
exercise
Sets Reps
Warm Up
Jog – 1500m Dynamic Stretching through full ROM
1- 1500m (Slow pace) High knees Christie Walks Deep Squad stretches Side to side Backwards run Touch ground slow run Kick ups
Interval Speed
40m Sprint
80-90% Max Progress intensity over time 15 reps
Accelerate/Deccelerate Straight line running.
20m Runs Cone to cone Progression Add 10m interval
Start 90% of Sprint 20 sets
Reaction/Agility Movement
Reaction Agility Box Jump down: Pass Ball/Header one direction on Cue Run other
20 reps x 2 – Run 10m Back.
Build fitness/Speed/Cardio
200m Sprint
5 Reps 80% Sprint
Sport Specific Shooting, passing skills – Off-balance progression with Pertubation
Shooting/Passing With Coaching team; Add Pertubation
N/A
Focus on Cutting Changing direction Progression add Ball
4D Cone Runs
15 resp/3sets/5x5x5
Warm Down
1500m Light jog Light Static Stretching recovery
1 Run Hamstring/Quad/add stretch Stretch for recovery as needed.
Sport Specific-Perturbation-Stability
Week 8-11
Goals: Progression
Stability – Perturbation+C:C
exercise
Sets/Reps
Increase HR
Warm- up – Cycling
15 mins
Functional dynamic activation
3- step Hold stabilise Backwards and foreword High Knee skips Back Pedals Lateral side to side Single leg alternating holds Single leg lift
Functional Movements, 20m Each
Achieve balance, stability Advance with Verbal Cue for which cone
Single leg Bosu exercise Balance – 1 leg Reach and touch cones
30 second x 10 reps
Stability, with unexpected force.
Step Down with Perturbation
Reps 15 Sets 3.
Progress to One Leg
TRX Forward facing full body Flexion.
Reps 15 Sets 3
Functional/dynamic Stability
Tennis football- All fours – Competitive Non-contact game
1 minute: 5 Sets
Resistance band, while performing Soccer skills to mimick opposition off balancing
Perturbation: Side/fwd/back Mvt Passing Shooting
1min x 5rep Each drill
Functional Specific Skill – Build confidence
Shooting Session with Goalkeeper
15 mins
Sport Specific, agility, speed, accelearation, deceleration, passing
Jog Pass, Sprint, to cones in different directions
15 mins
Warm down
Warm Down – slow cycle Passive stretch/Foam roller
10 mins
Return to Sport Assessment
Return to sport testing and assessment should be conducted through an objective analysis of lower limb strength, functional kinematics as well as ability to integrate to specific demands of the sport. Physiological (39) and psychological readiness also play a significant role. (32) Isokinetic strength of Quadriceps and hamstrings, as well as hop tests described in initial assessment should have >90% co-symmetry. (40) (41).
Tuck Jump and single leg squat assessments can be used to test asymmetries. (42)
For the Psychological component we can use the “12-Item ACL-Return to Sport (ACL-RSI) scale”. (39)
Sport Specific readiness assessed through systematic increases of load and subjective monitoring, of sport specific functions movement, and fitness levels.
___________________________________
Week 12 – If player has passed all tests – Resume training with Team – A multi-disciplinary approach with a Sports Psychologist for mental readiness of athlete in process would be ideal.Evidence based Approach of ACL Rehabilitation without surgery – Identification and progression of “Coper” with Conservative management
Author:
Constantinos Hadjichristofis – Bcom Human Resource Managment (Wits) PT (ACSM) BSc (Hons) Physiotherapy (Herts) MSc – Sports Medicine, Exercie and Health (UCL).
Osteoarthritis is characterised by a chronic and progressive degeneration of the cartilage of the joints. Although it often is seen predominantly in older adults, it can also affect younger population groups. It is often referred to as degenerative joint disease and its genesis and continued progression is often described as a “wear and tear” disease. As the cartilage breaks down, we see changes too in the underlying bone. Osteophytes can develop over time, also referred to as “bone spurs” that make the hinge of a joint, stiff and can be accompanied with pain and decreased mobility. Despite this, however properly prescribed and modulated exercise can help reduce the progression of Osteoarthritis. There are various exercise interventions that can positively influence the progression of Osteoarthritis, and even conserve joints, reduce pain and improve joint health in the long term.
Often individuals diagnosed with osteoarthritis develop fear avoidance behaviour of exercise, as there is a held belief that the cause of their osteoarthritis is their previous physical activity. In part, there is some truth. Competitive athletes in various sports, always have a risk for injury and substantial sheer forces. Competition either at the elite level or even the less conditioned athlete pushing their body to their peak individual performance can have a toll on the body and most certainly can be correlated or even the cause of earlier degeneration of joints. Sports by its very virtue is braving the chaos of unpredictable movements in the competitive setting, against unpredictable and chaotic resistance. There are indeed some correlative studies that certain high impact, contact sport athletes like Rugby players have a stronger pre-disposition to early onset osteoarthritis compared to the general population. However, that’s not the full story. The more important question is why, and what dynamics and forces cause the imbalances and ‘wear and tear’. We will explore the reasons, and what we can do to benefit from exercise safely and efficiently.
In order to do this, we need to first consider the genesis of the condition.
Heritability:
Of those that undergo hip and knee replacements, we find that their siblings also have an increased heritability risk profile, at a rate of severe Osteoarthritis being 27% (Chitnavis et al., 1997).
Mechanical Abnormality:
Mechanically abnormal joints have an unnatural distribution of forces. These can cause, more “wear and tear” without the inherent ability to adequately dissipate loads. Some conditions may be congenital (Genetic at birth). Some common disorders include Calve-Perthes disease (Hip Abnormality) and slipped upper femoral epiphyses (Molloy and Molloy, 2011). Hip Dysplasia is another factor that is an independent predictor of osteoarthritis, that if identified early, and corrective procedures can help reduce the long-term wear and tear from dysfunctional movements (Jacobsen and Sonne-Holm, 2005). Acetabulo-femoral impingement can also lead to eventual wear and tear of the hips, and subsequently limited movement dynamics in the hip joint, could also create increased stress in the knee and its mechanical forces.
Mechanical Injury:
Exercise although protective of the joint. Indeed, recreational runners showed no increased risk to non-runners in hip and knee osteoarthritis over 9 years (Jomha et al., 1999).
Increasing muscle strength as well as proprioception as well as reduced body mass index are joint protective. This protective effect is however lost in elite contact athletes not because the exercise itself is maladaptive, but due to the extreme nature of competitive sport, higher prevalence of injury and the ability to push their performance through pain, and this has an even bigger effect in contact sport. (Cheng et al., 2000)
Football players (Soccer) with previous ACL injury have an increased risk of developing osteo-arthritis (Jomha et al., 1999). We have a similar trend in meniscal injury, where there is a significant predisposition to the development of osteoarthritis post meniscal injury (Badlani et al., 2013). Sheer forces of a compromised meniscal knee have up to 8 times the sheer force load when the meniscal structure is compromised. This is compounded with high impact exercise such as plyometrics or other extreme forms of loading, like explosive pivoting and changing of direction (Lento and Akuthota, 2000).
Safe Exercise & why it’s beneficial in maintaining Joint health (Knee and Hip):
Exercise that is tailored, to gradually increase loads, in safe isolation yields substantial rewards in joint health. If the risk of injury is reduced through good foundational isolation muscle strengthening, as well as proprioception balance and stability – the global movers and local stabilisers, can decrease the load acquisition in the knee as well as the hip joint. Decrease in BMI also has a correlative effect on joint health. Exercise procures well-functioning lubricated joints (Fentem, 1994). The Joint itself is surrounded by the synovial membrane which produces a fluid that acts like a lubricant which allows joints to move past each other smoothly. Exercise is important in allowing for efficient distribution of this fluid. Exercise helps blood flow, and to distribute oxygen across important structures, as well as nutrients. It is also postulated in some research in mice that join-repair genes are activated that have some role to play in preserving joints (Lapveteläinen et al., 2001). Autophagy, is a process whereby damaged cells can be broken down and removed and this is also incentivised by exercise (Zhang et al., 2019).
Injury Prevention
Injury is indeed one of the mechanisms that is corelated with Osteoarthritis and the degeneration of cartridge due to the mechanical insult to the natural forces of the efficient biomechanical knee and hip. The goal for the Osteoarthritis patient should indeed be to reduce their risk coefficient of eliminating mechanical Injury in their exercise. Carefully modulated, strengthening, stability, proprioceptive training is vitally important in safely adapting to exercise for the osteoarthritic patient. It is therefore suggested that patients who are Osteoarthritic tread carefully and even avoid where possible high risk contact as well as working at maximum loads at the extremes of exercise performance.
Strategies in Exercise and a Biopsychosocial Approach:
Incentivising and promoting exercise is not always an easy task in the general population, especially in Osteoarthritic cohorts whereby there is a long held false belief that exercise is causing their osteoarthritis and degeneration. Exercise can have the potential however of joint degeneration and therefore suggestions to decreases loads under tension in unpredictable movements is warranted. We need to hypertrophy muscles, build stabilisation and proprioception without negligently overloading the joints. Some suggestions which will be discussed below, include Blood Flow Restriction (BFR) training; Isolation safe exercise at higher repetition maximums; meditative self-improvement mindsets over competitive, as well as flow and ‘play’ exercise groups for those who still want to engage in their favorite sporting activities.
Isolation exercise helps in muscle strengthening and hypertrophy, in the ranges of 8-12 Repetition maximums. At the range of 15-20 rep maximums (Baz-Valle et al., 2021) for conditioning and endurance which is a good place to start.
The muscle working in isolation and in a single plane of movement leads to safer more, predictable force outputs for safe muscle building. Eccentric exercise refers to muscle lengthening or the “negative”. These exercises are often shown to elicit a great protective response in stable forces as the muscle lengthens. Isometrics (no elongation or contraction of muscle) can also engage and activate a muscle early on safely (Anwer and Alghadir, 2014) (Pua et al., 2009).
Stability work on uneven surfaces serves a significant injury prevention and ability to stabilise and work on muscular proprioceptive ability.
Sport Specific, Flow and Play
An individual with osteoarthritis may want to progress to previous activities of daily living after an osteoarthritis diagnosis. This can be possible based on the parameters of the sport, what is required, and an athletes ability to mitigate risk through sport specific training and adaptation. Exercises must progress from isolation-exercise, to multiple plane and muscle recruitment dynamic exercise that safely replicates the demands of desired sport. Although certain levels of performance may be unreachable in safety, others can be worked towards if we adjust the social contract of sport, and bridge away from competitive mindsets to the mindset of exploration and mutual play, or flow. A fully competitive athlete with early onset osteoarthritis will have to honestly negotiate risk/reward, financial or otherwise of continuing in pursuit of top level performance with his longer term health through discussions with his medical team and coaches. Unfortunately, elite level sport does indeed have a correlation with progression of osteoarthritis and possible injury.
Suggested Exercise that is inherently friendly to Osteoarthritis
References:
ANWER, S. & ALGHADIR, A. 2014. Effect of isometric quadriceps exercise on muscle strength, pain, and function in patients with knee osteoarthritis: a randomized controlled study. Journal of physical therapy science, 26, 745-748.
BADLANI, J. T., BORRERO, C., GOLLA, S., HARNER, C. D. & IRRGANG, J. J. 2013. The effects of meniscus injury on the development of knee osteoarthritis: data from the osteoarthritis initiative. The American journal of sports medicine, 41, 1238-1244.
BAZ-VALLE, E., FONTES-VILLALBA, M. & SANTOS-CONCEJERO, J. 2021. Total number of sets as a training volume quantification method for muscle hypertrophy: a systematic review. The Journal of Strength & Conditioning Research, 35, 870-878.
CHENG, Y., MACERA, C. A., DAVIS, D. R., AINSWORTH, B. E., TROPED, P. J. & BLAIR, S. N. 2000. Physical activity and self-reported, physician-diagnosed osteoarthritis: is physical activity a risk factor? Journal of clinical epidemiology, 53, 315-322.
CHITNAVIS, J., SINSHEIMER, J. S., CLIPSHAM, K., LOUGHLIN, J., SYKES, B., BURGE, P. D. & CARR, A. J. 1997. Genetic influences in end-stage osteoarthritis: sibling risks of hip and knee replacement for idiopathic osteoarthritis. The Journal of bone and joint surgery. British volume, 79, 660-664.
FENTEM, P. H. 1994. ABC of sports medicine: benefits of exercise in health and disease. Bmj, 308, 1291-1295.
JACOBSEN, S. & SONNE-HOLM, S. 2005. Hip dysplasia: a significant risk factor for the development of hip osteoarthritis. A cross-sectional survey. Rheumatology, 44, 211-218.
JOMHA, N. M., BORTON, D. C., CLINGELEFFER, A. J. & PINCZEWSKI, L. A. 1999. Long-term osteoarthritic changes in anterior cruciate ligament reconstructed knees. Clinical Orthopaedics and related research, 188-193.
LAPVETELÄINEN, T., HYTTINEN, M., LINDBLOM, J., LÅNGSJÖ, T., SIRONEN, R., LI, S.-W., ARITA, M., PROCKOP, D., PUUSTJÄRVI, K. & HELMINEN, H. 2001. More knee joint osteoarthritis (OA) in mice after inactivation of one allele of type II procollagen gene but less OA after lifelong voluntary wheel running exercise. Osteoarthritis and cartilage, 9, 152-160.
LENTO, P. H. & AKUTHOTA, V. 2000. Meniscal injuries: A critical review. Journal of Back and Musculoskeletal Rehabilitation, 15,55-62.
MOLLOY, M. G. & MOLLOY, C. B. 2011. Contact sport and osteoarthritis. British Journal of Sports Medicine, 45, 275-277.
PUA, Y. H., WRIGLEY, T. V., COLLINS, M., COWAN, S. M. & BENNELL, K. L. 2009. Self‐report and physical performance measures of physical function in hip osteoarthritis: Relationship to isometric quadriceps torque development. Arthritis Care & Research, 61, 201-208.
ZHANG, X., YANG, Y., LI, X., ZHANG, H., GANG, Y. & BAI, L. 2019. Alterations of autophagy in knee cartilage by treatment with treadmill exercise in a rat osteoarthritis model. International Journal of Molecular Medicine, 43, 336-344.
Author:
Constantinos Hadjichristofis – Bcom HRM (Wits) PT (ACSM) BSc (Hons) Physiotherapy (Herts) MSc – Sports Medicine, Exercie and Health (UCL).
This article plans to examine and propose an efficient approach to strength-and-Conditioning for the boxing athlete to improve right cross (RC) punch efficacy. The RC is a full body movement with combined force coming from the ground through leg drive creating a kinetic chain and power generation transferred to the trunk and then the upper torso. (1)
Defining the Movement:
Starting from a relatively square hip-stance with slight angulation of the left hip forward. Both arms start at the head, elbows in. The punch comes from the posterior right hand driving the shoulder into slight protraction. Elbow is kept flexed and attached to the body until it crosses the hip line, before it is extended to complete the punch. (2)
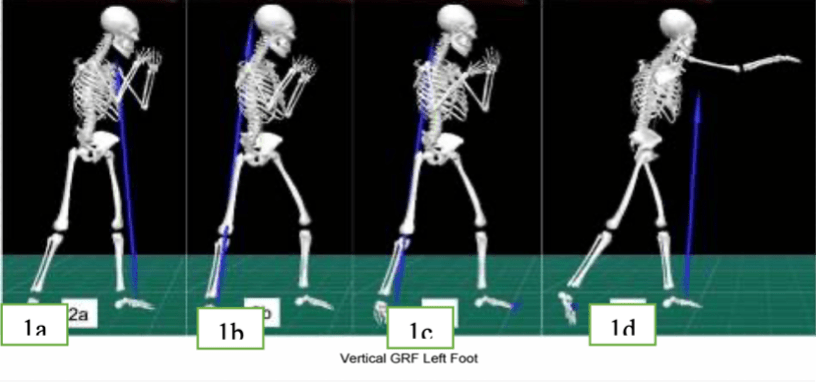
Rotational torque, and power, is generated through the connection to the floor. The right hip dips in the coronal plane, moves anteriorly in the sagittal plane and rotates internally. The left hip moves slightly downwards and backwards within the sagittal plane (Figure 1 and 3). (3-5)
The Right-cross (RC) is accommodated through 3 primary contributors: the arm, trunk and drive of the legs from the ground (6).
Figure-1 Right Cross Punch Phases Figure-2 Mike Tyson
The fundamental principle in boxing hinges on the notion that one maintains balance, whilst moving in such a way that one’s opponent is off balance. (7)
No single muscle is responsible for punching power in the right cross; It is a movement combination. The contribution of each muscle is presented in table-1. (8)
Table 1: Individual muscle groups – Eccentric, Isometric & Concentric function
Muscles (Concentric – Isometric – Eccentric)
Upper Torso
– Pectoralis Major (adduction, internal rotation, flexion of humerus and shoulder joint . Involved in stabilizing the functional movement chain.) – Latissimus Dorsi (Often overlooked muscle, but of importance in keeping the punch tight, and allowing for transferal in biomechanic chain from the ground. Adduction, Extension and Internal rotation of arm. Aids in respiration, breath out on punch). – Teres Major (Assists the latissimus dorsi in adducting the humerus downwards and backwards – Important in stabilizing humeral head, and keeping tight kinetic chain, for transferal of power from legs.) – Trapezius – Brachii Lateral head; Triceps Brachii Long Head; Triceps Brachii Medius (Triceps muscles involved in the last initiation phase of action. Move alongside kinetic energy already created by the full body kinetic chain – guided by high velocity of body kinematics and other contributors- arm punchers with over recruitment of this muscle is inefficient) – Rotator Cuff (Subscapularis; Supraspinatus; Infraspinatus; Teres Minor). – These muscles form an important structure in stabilizing the shoulder. They perform some important functions including rotating the upper humorous internally as well as external rotation in getting back to the neutral position.- Anterior Deltoid – Is the main muscle that can work to increase power, working with the pectoralis major to concentrically create power generation and pull the shoulder into an efficient position for impact at end point of punch.- Bicep (Short and Long head of Branchii) – Although the biceps are involved concentrically in pulling the punch back and eccentric loading on hit, they are not the major power generator of the punch. But they help to facilitate the muscle sling involved in a punch.
Trunk
– Internal & External Abdominal Oblique (Ipsilateral rotation and lateral flexion of the trunk – Rotation of trunk to opposite side depressing thoracic cavity)- Serratus Anterior (Boxers Muscle – Draws scapula internally and forwards, aiding in protraction of shoulder, keeping punch tight as well as additional torque)- Transverse Abdominus (Involved Isometrically in stabilizing and keeping the kinetic chain and power transfer intact as it comes from the ground)- Rectus Abdominus (compression of abdomen, trunk flexion with stabilization – aiding in RC power transfer).
Lower Torso
– Gastrocnemius (Initiates power and movement, boxer on toes, facilitates drive – contralateral front gastric eccentrically absorbs load and maintains balance.)- Gluteus Maximus (Rear: Prime mover in hip extension, used in proximal range, then other antagonist muscles take over)- Gluteus Medius (Slight abduction of hip, and stabilization of the pelvis, anterior fibers engage for internal rotation and flexion.)- Rectus Femoris (Flexion of Hip joint – recruited in proximal range on contraction in back leg- Lead leg then works eccentrically to maintain balance after punch thrown).- Biceps Femoris Right back leg (involved in added power by flexing knee and taking over from rectus Femoris as it is an antagonist muscle). Front leg, eccentrically loads at end range of punch.- Adductor Longus (Adduction and flexion of hip. Extension + Internal Rotation of femur. Pelvis Stabilization. Concentric activation, followed by eccentric stabilization at end of motion in back leg).
Boxing has a 70-80% dependence on anaerobic processes, 20-30% aerobic(15). Boxing RC activates type IIb/IIx myosin fibers which enable high speed contraction for maximum force. (16)
Muscle fibers include a combination slow fatigue resistant (Type-1) and fast twitch, high hypertrophy, explosive Power (Type 2) fibers. (17)
The sliding-filament theory explains how muscle fibers are stimulated. An actin filament glides over the myosin filament. The length of filaments does not change when the muscle is contracted, however the length of the sarcomere is decreased as the actin moves and glides past the myosin filaments. The z-discs in turn are pulled towards the center of the sarcomere. (20) This is shown in figure 3 below:
Figure-3 Graphical Illustration of pre/post contraction of muscle fiber.
From Relaxed state, to Maximal Power Generation and back
Delvechio suggests that the traditional high aerobic mindset in traditional boxing trainers, must be replaced with stronger influence in anaerobic strength and conditioning rather than aerobic protocols. (23)
Type-1 fibers also play a fundamental role. The boxer needs to maintain his balance, in constant motion. (24) Type-1 fibers activated and relied upon with regards to keeping good posture and a solid balanced stance at all times. (13)Bruzas et al. point out that aerobic fitness in boxers is directly correlated with the rankings of professional boxers. (25) It should be concluded that in the RC movement, good aerobic fitness and stability control is of vital importance in maintaining the balance required, to best be able to execute the RC with fluidity and from an energy conserving state, to generate explosive power of the RC at an opportune time. (26)
As the explosive power of the punch mechanism, shouldn’t leave the boxer out of postural position at any time the boxer can’t rely only on anaerobic contractions of type-II muscle fibers and constant high output contraction through the entirety of several 3-minute rounds (2).
The natural stretch shortening cycle (SSC) is important and is engaged in a functional combined movement such as the straight-RC. (6) The dynamic involves an eccentric stretch of the agonist muscle followed by a rapid shortening in the concentric phase, creating more power in the punch. (1) This is known as pre-stretch. It has a reflex component that acts like an elastic band. When stretched it snaps back. This is a counter movement component, which increases the ability to utilize a stronger velocity/power mechanism. It is further observed that eccentric strengthening improves performance in the SSC (27). This is also seen in the elbow. As shown in Figure 4, we see a pre-eccentric stretch reflex before the rapid concentric firing stage in the elbow.
Figure-4 Pre-Stretch Eccentric loading before Concentric max power: Elbow Displacement.
With regards to the upper torso, one of the mechanisms of power generating concentric extension of the humorous would be the pectoralis major and anterior deltoid. (Fig.6)
Figure 6 – Function of pectoralis Major and Anterior Deltoid ) Incline-press.
Lopez (11) explores the relationship between bench press(BP) and punch RC performance. Although Correlation is found between 1RM max performance in BP and punching power, the effect and direct influence is speculative due to low specificity of the complete movement and technique of the athlete. The right cross is an asymmetrical motion and the bench press is not. Irrespective however, stronger punchers of the RC had better BP outcomes. Power generated from a relatively isolated muscle as exhibited in the BP can be correlated to power and punch efficacy of the RC. Overload of the muscle even in non-sport specific exercise creates applicable RC power. (29)
Filimonov et al. analyzed 120 boxers, showing that as experience and competitive level of the boxer increased, so did the amount of force contribution from the lower trunk. (30) Giovani and
Nicholas show that amateur boxers, with higher maximal power in the legs, derived higher maximal force in the upper limbs. (10)
It is however important to note that the end point of contact is the upper limb. And for the power of the legs to effectively be transferred to the upper limb, balance technique and stability become primary drivers of delivery as shown in Figure 5 & 7.
Fig-7 – Key Drivers of Punching Power
A performance exercise program must focus on strengthening the significant systems that best allow the athlete to benefit from mechanically correct movement.
Guidetti (31) also points out that grip strength is also correlated with increased total power efficiency in the RC as it allows for Isometric contraction and stabilization in transferring energy from ground to upper extremity, highlighting the importance on full system stability, and training with an emphasis on power generation.
The Force Velocity curve is show in figure-8. The inverse relationship between force and velocity shows us that when force output is maximized slower movement is produced. To increase power, we need to consider both Velocity and force and the prescribed exercise needs to compromise of both movement and load. (12) Trade-off between force and velocity is believed to happen because there is a decrease in time for cross bridges to be able to form in high velocity exercise. More cross-bridges are associated with a greater contractile force. Slower velocity/high force exercise allows more time for these cross-bridges to be formed, (32) however has the opportunity cost of reduced muscle contractile velocity. (33)
Yoon et al. (14) show that isometric trunk-strength is associated with anaerobic power and maximal strength.
Professional boxers emphasize power generation and hit harder often from a closer distance, whereas Amateur boxers, tend to hit more punches at end range, with more focus on velocity and speed, rather than power generation. This can be attributed to scoring and rule differences and the fact that knockouts are less commonplace in amateur boxing with a greater emphasis on points. (12) This highlights the importance of the length-tension relationship in generating force in the RC. The length-tension relationship dictates that isometric tension in the muscles is indicative of the amount of cross-over of actin and myosin filaments (Figure-9). This shows, us that pure force generation does not come at end range of the punch, but at mid-range. (34)
Figure-9 Length-Tension relationship of Sacromeres presented in graphical form
Each athlete, should be assessed in a comprehensive SWOT (Strength; Weaknesses; Opportunities; Threats) (36)analysis (37). Case-Study A (Appendix) wants to focus on Power Generation of an already conditioned athlete. This is a middle-weight boxer, and we do not want to hypertrophy. We will use the overload principle and 80% of 1RM 4-6 sets for power gains with increase in resistance every week for the first 6 weeks. (38) Our periodization will focus on Macrocycles (38), based on the length from the event and the coaches periodization cycle based roughly around USOEC Guidelines (39). Our strength and conditioning program to improve RC power is designed to fit into the athlete and coaches boxing training regimen.
The boxer should ideally go through 4 cycles: “preparation, general strength, pre-competition and active rest” (39). Our program has been included in the boxers ‘General strength’ (16 weeks pre-competition) and ‘pre-competition’ phase. (10 Weeks pre-competition). Each phase runs for 6 Weeks. This has been done as boxers should not periodize with a strength/power focus 6 weeks before Competition. The next 6 weeks we have included plyometrics to increase velocity and speed and less emphasis on power. (39) We have then allowed for 4 weeks pre-competition for exclusive focus on boxing specific training with their coach. The active-rest cycle happens after competition. It is intricate that boxers feel confident and have some familiarity and confidence in their training regiment, as the psychological burden of entering a fight cannot be understated. (40)
Conclusion
Developing a generic approach to inherent power in the RC has evaded boxing experts and SC coaches for years. This is likely due to the fact, that it cannot exist in a movement as complex as the RC in boxing with athletes of different genetic traits. The approach must be focused on individualized assessment of the individual athlete and a boxing program prescribed based on a SWOT analysis, and multidisciplinary team.
27 year old professional middleweight Boxer A seeking a strength and conditioning program to improve efficacy of his right cross in upcoming fight in 16 weeks against Boxer B
Subjective Assessment:
Multidisciplinary meeting with coach and athlete. Utilization of SWOT analysis as recommended in article.
Stengths
Weaknesses
Boxer A
Superb Aerobic conditioning. Workhorse, Road Warrior. No problems into later rounds. Great Point fighter. Fast and technical. Good core strength. Creates openings to land power shots. Good velocity on punch. Great defensive skills, runner, able to evade well.
Has trouble finishing opponents despite great technical openings and landing shots. Balance stabilisation can improve in overloading power punch.
Boxer B
Gets stronger as fight progresses. Relentless forward pressure. Dangerous power through fight. Power Puncher. Many later round knockouts. Willing to trade to get shots in.
Opens guard to trade. Can be slow in movement.
Opportunties
Threats
Boxer A
Evasive and movement superiority.Many opportunities to get power shots in whilst evading.Early power shots, may slow down opponents forward pressure.
Facing power puncher. Relentless forward pressure and danger of knockout.
Boxer B
Foreward pressure can tire opponent early. Can take punishment but wins trades due to power.
Unable to return punches against runner, with respectable power.
Goal of strength and Conditioning program based on Gameplan:
Coach and Boxer A have decided, that the strategy for upcoming fight, is to increase power of right cross, whilst maintaining balance, and stability/movement. The game plan, is to keep distance and punish pressure boxer B with a running game, but improve power output utilizing Boxer A’s Running and evasive style, at a safe distance without trading punches. (Right cross is a long range punch).
We have decided to incorporate a 12 week strength and conditioning program based on this goal, that will be incorporated into the boxing training protocol. There will be 4 sessions a week dedicated to this goal, for 12 weeks. First 6 weeks, will be dedicated to power and strength of upper and lower body. The following 6 weeks, will add plyometric exercises. Program will also develop eccentric and Isometric stabilization as increased power in punches will have more demands in eccentric capacity to pull punches back and move. These exercises will be fit into the regular boxing workout protocol with the coach, and will form a part of the strength and conditioning regiment.
This will be followed by a twice a week ‘maintenance’ period of gains in the final 4 weeks leading up to fight day, where Boxing technique, recovery and other aspects of training will take priority.
Warm-Up/Replacement activity to Increase HR
15 minutes rope skipping Depending on Upper body lower body, athlete preference.
Warm-Down
10 Minutes Skipping.
10 Minutes Stretch or Ice Bath.
Notes:
Program has been created, to fit into the athletes Boxing Specific program. The boxing coach will increase heavy bag work, and maximum output pad work.
The purpose of this program is to create the ability to overload the athlete increasing strength and power. Plyometric days are added from week 6-12, to keep velocity speed. We have also focused on several core stabilization exercises.
We want to focus on Power Generation of an already conditioned athlete. This is a middle-weight boxer, and we do not want to hypertrophy. We will use the overload principle and 80% of 1RM 4-6 sets for power gains with increase in resistance every week for the first 6 weeks. (38) Our periodization will focus on Macrocycles based on the length from the event and the coaches periodization cycle based roughly around USOEC Guidelines (39). Our strength and conditioning program to improve RC power is designed to fit into the athlete and coaches boxing training regimen.
The boxer should ideally go through 4 cycles: preparation, general strength, pre-competition and active rest (39). Our program has been included in the boxers ‘General strength’ (16 weeks pre-competition) and ‘pre-competition’ phase. (10 Weeks pre-competition). Each phase runs for 6 Weeks. This has been done as boxers should not periodize with a strength/power focus 6 weeks before Competition. The next 6 weeks we have included plyometrics to increase velocity and speed and less emphasis on power. (39) We have then allowed for 4 weeks pre-competition for exclusive focus on boxing specific training with their coach. The active-rest cycle happens after competition. It is intricate that boxers feel confident and have some familiarity and confidence in their training regiment, as the psychological burden of entering a fight cannot be understated.
Program First 6 Weeks – Phase 1 – Strength/power acquisition Isolated movement:
Weeks 6-12: Addition of Plyometrics, Sprints and whole body movements. Monday and Thursday. Adaptation for utilising Power gained from week 1-6 into a more Velocity and functional movement, but maintaining Power on Velocity/Force Curve.
Wk 6-12 Tuesday & Friday: Full Body Gym Work.
4 Weeks Remaining before fight: Focus on Boxing Specific work only with Boxing Coach. Emphasis on game-plan, and adopting full power pad work and heavy-bag work. Safe zone to adapt and peak workload, or maintain according to how athlete is progressing.
Author:
Constantinos Hadjichristofis – Bcom Human Resource Management (Wits) Personal Trainer (ACSM) BSc (Hons) Physiotherapy (Herts) MSc – Sports Medicine, Exercise and Health (UCL).
Physical Therapy, dates back to the ancient world. There is history throughout China and Ancient Egypt as well as ancient Greece. One of the most famous practitioners of using movement as well as non-invasive manual techniques as holistic medicine is Hippocrates himself, who also has originated the oath that all medical physicians still swear to. There is recorded history of manual adjustments, hydrotherapy and efficacious restorative movement attributed to Hippocrates. These records date back as early as the 4th century BCE (Sharma, 2012).
Modern Physical therapy began taking shape as a formal entity in the 18th century. This came as a consequence of advancement of Orthopaedic medicine. Pioneers included the Royal Central Institute of Gymnastics in 1887 which had recognized the term Physiotherapy” under the auspices of Sweden’s National Board of Health welfare. Subsequently Nurses had established the first organisations geared towards physical therapy treatment. The modern day CSP – (Chartered Association of physical Therapy) in the United Kingdom was first founded by four nurses in 1894, and was awarded its Royal Charter in 1920 (CSP, 3 August 2020).
Moving towards the 1960s and even towards the 1990s, physical therapy went through various stages. Initially the profession was physician led through standard protocols and practise. Early Physical therapists followed guidelines strictly for each injury and clumped many different individuals with similar presentations together in facilitating standard protocols. Through this mode of practise many physical therapy “gurus” also emerged, whereby the profession was elicited through passing down of knowledge in an apprentice procurement of services. Big Gurus through succinct marketing, and experience, taught many seminars. Certifications were common practise amongst these ‘treatment styles’. Unfortunately, many physical therapists are still trained in this mindset, of procurement of certifications through institutions that are not explicitly evidence based. Even today the highly discredited “Bowen” technique is often being promoted across Cyprus. Even the Cyprus association of physical therapists is promoting and hosting seminars on these largely defunct “Gurus”.
Modern day physical therapists especially with regards to standard practise in the UK, Netherlands, USA, South Africa and Australia are trained explicitly as Allied Health care professionals. They are introduced to evidence-based practise. Physical Therapy as a profession, now has its own publications and evidence-based studies coming out every day, on standard of care. As we see in Figure 1 there is a hierarchy of evidence. From expert opinion (old school gurus, which forms the bottom and least significant evidence), to Case control studies, cohort studies, Random controlled trials, Critically appraised individual articles, and finally into Systematic Reviews, that help procure the most established evidence based practise.
Figure 1
Physiotherapists are now taught, to work as a cohesive multidisciplinary team (figure 2), with physicians, nurses and other health care professionals with the patient, and his individual presentation at the centre of it all.
Figure 2
Figure 3
Evidence based research is introduced at undergraduate level in the UK syllabus. Research Methods play an important role in the modern-day physiotherapy syllabi. At Post graduate levels students present their own research in a topic that interests them. In the 21st century, with an abundance of information, it is also important to understand that the English language, is the language of the academia. The inability to communicate efficiently in this language, allows for marketeers, gurus and also organisations to promote various low efficacy modalities, as efficacious treatment modalities, which actually have very little efficacy in the literature, if at all, with some extremely low-quality studies.
Without succinct training in Evidence based practise, we unfortunately end up with organisations in Cyprus like that of PAP (Pancyprian Association of physical therapists), that are promoting seminars in pseudoscientific modalities like Bowen. Bowen himself, has no formal medical training, and succinctly described his approach as a “gift from god”. He died as an unlicensed practitioner and did not even qualify as an osteopath (Which also is not part of allied evidence-based health care professionals).
“In 2015 the Australian Government’s Department of Health published the results of a review of alternative therapies that sought to determine if any were suitable for being covered by health insurance; Bowen Technique was one of 17 therapies evaluated for which no clear evidence of effectiveness was found (AO, 2015).”
And yet even in 2022 the Cyprus Association of Physical therapists is promoting quackery and pseudoscience. Indeed, in last trimester a Bowen seminar and a needling seminar, were the only promoted seminars for physiotherapists presented and made available.
The problem in Cyprus however is that often many leading Physical Therapists are not practising Evidence based physical therapy. Many are still following pseudoscientific modalities, based on marketing, and the ability of such organisations to release translated procurements of information to health care professionals only speaking Greek. It is a tragedy that an association that is meant to be part of an evidence-based profession, part of the allied Interdisciplinary team has no regard for evidence-based practise.
This is why foreign memberships like the UK’s HCPC and CSP are of importance. Unfortunately, the PAP (Pancyprian Association of Physical Therapists) needs to do a better job in promoting evidence-based practise.
AO, C. B. 2015. Review of the Australian Government Rebate on Natural Therapies for Private Health Insurance.
CSP. 3 August 2020. CSP History- Founded by four nurses in 1894, the CSP was awarded its Royal Charter in 1920 and has become the profession’s leading membership organisation in the UK. [Online]. [Accessed 21 February 2022].
SHARMA, K. N. 2012. Exploration of the History of Physiotherapy. Scientific Research Journal of India, 1, 19-22.
Exercise Promotion Saves lives, promotes long term health and the astute failure of the Cyprus Education system in promoting exercise, and the deleterious effect of scaring children from play and Exercise.
Misinformation, often comes part and parcel in the current landscape of the internet, main stream media networks who have specific contributors, political goals and other moving processes. What is less common, but an extremely worrying trend, is for an intentional psy-op designed specifically in such a way that can do monumental harm to children, their health and their development.
The book that was set as a set work in Cyprus for kids aged, 5-8 years old, titled: “No! You won’t get in our nose”, has done just that. It coercively insinuates and tells children to not fall victim to “mind control by aliens” which are trying to fool them into “play” (Exercise), fresh air and sunlight, because these aliens want to artificially inseminate the kids with disease designed, and targeted to kill their parents (referring to COVID-19 ofcourse) (Figure-1).
Figure- 1
This science fiction author, dubbed the Roahl Dahl of Greece and Cyprus – Evgenios Trivizas, has done something remarkably dishonest with his story and connections in being able to administer such a book into the Cyprus education system as a set work, in programming kids, into fear-avoidance behaviour and triggering anxiety disorders when presented with exercise and play (1). It’s amazing how a sociologist can have so little knowledge, training, or any scientific idea of the impact of such actions long term in children. The same children, who have faith, belief and goodness. The same children who grow a large smile every year in Christmas eagerly awaiting Santa Claus. Children who are easily exploitable into dysfunctional beliefs, that will affect them and scare them towards unhealthy lives, and a lifestyle of long-term detrimental ills. Not to even mention long term symptoms of PTSD should the narrative in any way come true if they were to infect their parents with COVID and having a negative outcome. The blurring of the lines of fact and fiction, to cause immense paranoia and a dishonest distortion of reality. So, let’s delve deep into the science of sport medicine exercise and health and the true implications of what this ignorant and frankly dangerous author has tried to coerce innocent kids into and the severe long-term ramifications.
Exercise, play, human interactions are absolutely vital for the efficacious development of the adolescent and child (2). There is efficacy and positive impact throughout the entire duration of a human’s natural lives. The developmental periods in children have to be emphasized as the consequences can be truly life changing. There is a large body of scientific evidence which unequivocally indicates the important nature of exercise and play in children. This is not an opinion piece; this is a fundamental and bedrock truth based on exhaustive consensus of medical scientific literature. In fact writing this paper is burdensome in that, this should be blatantly obvious to any governing body, institution or ‘sociologist’ whose aim is to mould the behaviour of children. Yet here we are, trying to desperately bring sense to the corrupt and incompetent bodies in charge of child education in Greece and Cyprus.
Sensorimotor and Cognitive Influence
Increased exercise facilitated through play not only drastically improved manual dexterity, aiming and catching skills, and static dynamic balance as one would expect, it was intrical in promoting motor and cognitive development. (2) Exercise Intelligence plays a fundamental role in the formation of the child’s brain, and has absolutely long-term effects that can last a lifetime in this critical period. As published in the Journal of Psychology Sport and Exercise, Ellemberg et. al conclude: “Exercise has a beneficial impact on different aspects of brain functioning during development. Indeed, both sensori-motor and cognitive functions are ameliorated.” (3).
Osteoporosis Bone health and exercise
Below in figure-2, is a slide presented by Dr. Richard Keen in 2019, a senior Consultant Rheumatologist and honorary Senior Lecturer at University College London.
Figure-2
As shown above a slow loss of bone mineral density begins at around age 40. From the age of 25-40 we have a consolidation phase of peak bone mass already acquired, in the integral years from 0-25 years.
As is evidence and common knowledge in all scientific literature bone mass acquisition has a very important and direct correlation with weight bearing, exercise and sunlight (Vit-D levels) (4).
It is therefore essential for children, to engage in active exercise and play in these integral years, as the bone mass established here, can last a lifetime. Although we can reduce bone loss with weight bearing exercise in later years, we can not revert the opportunity cost lost in the most important years which is from 0-25 yrs. This categorically shows how intricate the child’s developmental years in forming good Bone Mass and bone health and also avoiding conditions like osteoporosis in later years.
Vit D Levels – Covid Risk – Exercise outside contributes to combating Vitamin-D deficiency
It would also be important to mention here, that Vitamin D adequate levels also reduce serious infection, hospitalisation death and even replication of covid drastically, as shown in this recent peer reviewed study out of Israel (5). Indeed, creating fear-avoidance in children to exercise outside, and partake in normal activity, would increase the risk of transmission to covid. People who are vitamin D deficient are 14 times more likely to have severe COVID-19 and to die from the disease, according to research from scientists in Israel. “The peer-reviewed study, published in the journal PLoS ONE, looked at vitamin D levels before a person contracted COVID-19 and the disease’s severity and mortality. The latest study is among the first to look at vitamin D levels before a person contracted the virus. Researchers say this gives a more accurate assessment than when measuring vitamin D levels when the person is already being hospitalized for COVID-19, when levels may be lower due to the disease.” (5) Although one could argue, that on the individual level, Vitamin D could be prescribed orally to supplement and avoid Vitamin D level insufficiencies, it is important to note, that the Cyprus government has done a terrible job in promoting this, and beyond that, on a socio-economic macro level the promotion of Evgenios Trivizas book together with governmental policies by both the Health Minister of Cyprus and the active measures has an absolute, and detrimental effect in actively lowering vitamin D levels from lack of sunlight (6) and exercise. At the macro level, this is disastrous for the entire population, but even more so for Children at this very important developmental stage. The truth is that these ill-educated policies have killed thousands of people across the world, from both primary and secondary factors, and will continue to drastically impart a negative affect on health for years to come (7)(8).
Child Obesity rates in Cyprus of grave concern
Child obesity rates in cyprus are comparable to that of North America, that’s an obesity rate of 10,3% in males, and 9.1% in females. (9) Paediatric obesity requires individualised as well as population wide measures to promote exercise and efficient diet. (10) The misstep by both government, and schools scaring children away from exercise will have huge ramifications in the future, which can lead to increased obesity rates, type-II Diabetes and even metabolic sydromes. This is a pandemic that can-not be ignored. These population groups have also been shown extensively to be more at risk for hospitalisation or death. Specifically, regarding children there are extremely few if any severe cases found in children without co-morbidities resulting in ICU respiratory support or death. (11) (12).
Fatness Fitness and Increased Cardiovascular risk in young children
Body fat with emphasis on its distribution plays an important role in cardiovascular risk in children. More so than even cardiorespiratory fitness. In the healthy cohort however, children with better cardiovascular fitness still elicits a relevant protective effect from metabolic risk (13).
Diabetes Exercise, Children
According to current ADA (14) standards children both diabetic and pre-diabetic must undertake at least 60 minutes of moderate to vigorous aerobic activity every day as well as muscle and bone strengthening exercise 3 days a week. More activity, was correlated in a higher quality of life (14). Lockdowns, mandates, and a book to disincentivise exercise and play in children out of a fear response, once again is utterly negligent, and when observed at the macro scale will reduce QUALYS (Quality of Life years), increase mortality, and absolutely negatively influence health. If it was not enough, that schools were shut down; If it was enough that sports events shut down; If it was not enough that government school teachers in Cyprus often demand finishing their day at 1-2pm rather than facilitating sport. Now on top of that we have an author, who is trying to create fear avoidance of exercise in children. Exercise and play in children is the best medicine (15) (16) (17), and any attempt to make children categorically avoid it ‘for the health of themselves or parents’ is contrary to all scientific literature. Indeed, the hospitalisation or death rate from covid-19 to children is statistically less than significant. (12) However the toll of an unconditioned, unfit, obese youth is exponentially more dangerous, both today tomorrow and in the future.
Conclusions
Obesity, lack of physical activity and smoking are the top causes of premature deaths in the USA. (17) Cyprus impact is similar to North America. (10)
British Journal of Sports Medicine (BJSM):
“Evidence supports the conclusion that physical inactivity is one of the most important public health problems of the 21st century, and may even be the most important” – Steve Blair BJSM (18)
American College of Sports Medicine (ACSM):
Data suggest that more than two thirds of people would be more motivated to exercise if prescribed by their physicians, schools and public health bodies. (19)
Journal of the American Medical Association – (JAMA)
“Physical activity, while not a drug, can behave like one” – Health care professionals should prescribe physical activity, as should national health bodies. (20)
Cyprus & Greek Education Boards & Evgenios Tivrizas 5-8 yr old set work: ““No! You won’t get in our nose”,”
Aliens, are trying to mind control children to play, so that they can catch COVID, so they can kill their parents. Children should not be influenced by the aliens mind control initiatives, and avoid exercise and play (21) (22).
Final word
It’s time that people are held accountable for their actions. Parents should not only demand that this book be immediately discontinued as a child set work – but also that those who approved and gave the green light should be held accountable and the board in charge of establishing school set works be replaced.
As for the author Evgenios Trivizas.. free speech is a fundamental aspect of free societies. But ignorance can not be facilitated and indoctrinated on impressionable young minds.
_______
1. Hirshfeld-Becker DR, Masek B, Henin A, Blakely LR, Pollock-Wurman RA, McQuade J, et al. Cognitive behavioral therapy for 4-to 7-year-old children with anxiety disorders: a randomized clinical trial. Journal of consulting and clinical psychology. 2010;78(4):498.
2. Pesce C, Masci I, Marchetti R, Vazou S, Sääkslahti A, Tomporowski PD. Deliberate play and preparation jointly benefit motor and cognitive development: mediated and moderated effects. Frontiers in psychology. 2016;7:349.
3. Ellemberg D, St-Louis-Deschênes M. The effect of acute physical exercise on cognitive function during development. Psychology of Sport and exercise. 2010;11(2):122-6.
4. Eliakim A, Beyth Y. Exercise training, menstrual irregularities and bone development in children and adolescents. Journal of Pediatric and Adolescent Gynecology. 2003;16(4):201-6.
5. Dror AA, Morozov N, Daoud A, Namir Y, Yakir O, Shachar Y, et al. Pre-infection 25-hydroxyvitamin D3 levels and association with severity of COVID-19 illness. Plos one. 2022;17(2):e0263069.
6. Wacker M, Holick MF. Sunlight and Vitamin D: A global perspective for health. Dermato-endocrinology. 2013;5(1):51-108.
7. Ioannidis JP. Coronavirus disease 2019: the harms of exaggerated information and non‐evidence‐based measures. European journal of clinical investigation. 2020;50(4).
8. Melnick ER, Ioannidis JP. Should governments continue lockdown to slow the spread of covid-19? BMJ. 2020;369.
9. Savva SC, Kourides Y, Tornaritis M, Epiphaniou-Savva M, Chadjigeorgiou C, Kafatos A. Obesity in children and adolescents in Cyprus. Prevalence and predisposing factors. International Journal of Obesity. 2002;26(8):1036-45.
10. Savva S, Kourides Y, Tornaritis M, Epiphaniou-Savva M, Chadjigeorgiou C, Kafatos A. Obesity in children and adolescents in Cyprus. Prevalence and predisposing factors. International journal of obesity. 2002;26(8):1036-45.
11. Stavridou A, Kapsali E, Panagouli E, Thirios A, Polychronis K, Bacopoulou F, et al. Obesity in children and adolescents during COVID-19 pandemic. Children. 2021;8(2):135.
12. Ludvigsson JF, Engerström L, Nordenhäll C, Larsson E. Open schools, Covid-19, and child and teacher morbidity in Sweden. New England Journal of Medicine. 2021;384(7):669-71.
13. Suriano K, Curran J, Byrne SM, Jones TW, Davis EA. Fatness, Fitness, and Increased Cardiovascular Risk in Young Children. The Journal of Pediatrics. 2010;157(4):552-8.
14. Association AD. 5. Facilitating Behavior Change and Well-being to Improve Health Outcomes: Standards of Medical Care in Diabetes—2020. Diabetes Care. 2019;43(Supplement_1):S48-S65.
15. Sallis RE. Exercise is medicine and physicians need to prescribe it! Br J Sports Med. 2009;43(1):3-4.
16. Pedersen BK, Saltin B. Exercise as medicine–evidence for prescribing exercise as therapy in 26 different chronic diseases. Scandinavian journal of medicine & science in sports. 2015;25:1-72.
17. Berryman JW. Exercise is medicine: a historical perspective. Current sports medicine reports. 2010;9(4):195-201.
18. Blair SN. Physical inactivity: the biggest public health problem of the 21st century. Br J Sports Med. 2009;43(1):1-2.
19. Jonas S, Phillips EM. ACSM’s exercise is medicineTM: A clinician’s guide to exercise prescription: Lippincott Williams & Wilkins; 2012.
20. Lee I-M. Dose-response relation between physical activity and fitness: even a little is good; more is better. Jama. 2007;297(19):2137-9.
21. Theodoulou N. Coronavirus: Parents angered over ‘scary’ Covid schoolbook
Clinical reasoning, is imperative in the active assessment of the knee.
The examination should be composed of subjective examination and an Objective examination.
The subjective examination, is critical in getting to know your patient, his patient history, past medical history, medications. The process is intrical part of patient assessment, and an investigation into the nature of a patient’s pain or acute/sub-acute/chronic injury. It involves a series of questions, that make the patient an active part of his own treatment. The patient is always central. It’s a way to not only gauge the patient’s problem, and give vital information on the treatment approach, but also vitally important, in getting to know the patients short term and long term goals, intentions, activities of daily living. It is also an important bargaining process, where expectations of patient is listened to, and worked towards, but also simultaneously modulated and adapted to what is possible. Patient education is absolutely essential in this process, however what is even more important is to actually LISTEN to the patient, as he is the arbiter, and true hero in his rehabilitation story. We facilitate treatment, and enable evidence based intervention.
The Objective examination, involves a series of clinical reasoning, through standardised evidence based objective examinations.
The Objective examination of the Knee, involves beginning with general observation in standing. We look at static posture – Front, back and side. We observe for unnatural gait and any compensations.. It is important to distinctly observe and examine functional movement. We already spoke about gait, other functional movements, can include a squat, or/and a single leg squat. Clearing the joints above and below the knee is also essential.
Special tests of the knee are also vitally important. These are backed up with evidence-based literature, and we have values of specificity and sensitivity, through double blind control studies, and systematic reviews. Sensitivity refers to the ability of a test to correctly identify patients with a condition. Specificity refers to the ability of a test to correctly identify people without the condition. Special tests can detect certain abnormalities in the knee structure or pick up an acute or even chronic dysfunction. For example, if we suspect meniscal damage or tears from our subjective examination, we can do tests like mcmurrys, thessallys and other test to see the integrity of the medial and letaral meniscus. If ligament damage is suspected, we will test the integrity of suspected injury, for example the medial and lateral ligament integrity. Tests like the lachmans and anterior drawer test would be used to test the integrity of the anterior collateral ligament.
Anterior Drawer Test – ACL
Mcmurrys test – Meiscus
Lag Sign Observation – PCL
The posterior collateral ligament might present with an observable sag sign a positive posterior drawer test as well as the active Quad test. In all the ligament tests, we are looking to compare with the other healthy knee. We are looking for signs of instability in ligaments, and laxity, that would induce a hypermobile presentation. With regards to meniscal tear tests we may observe a replication of symptoms, locking, and deterioration of natural motion, reproduction of pain or apprehension. Posterior Lateral corner could also be tested for possible serious injury through a dial test.
Muscle tests could also help us distinguish other injuries to the knees, including muscle strains, tendonitis or other distinct mechanism or condition within the knee. Muscle strength tests could for example be examined in the Quads, hamstrings (90; 45; 10 degree static strength). Weakness could be indicative of reffered or neurologic in nature pain. Testing of active range of motion (Patients own movement) as well as passive range of motion of knee (Knee pasively moved by therapist). Ranges that are examined, include flexion, extension, Internal rotation and external rotation.
Palpation also plays a key role. Bony landmarks, joint margins, tendons, fat pad, muscle and Bursae can be palpated.
Patellofemoral joint should be observed, for efficient and smooth gliding and tracking (J sign; Clarks Sign). Pattela apprehension test, can be used, if there is pain and patient has a guarding behaviour.
J sign
Muscle legth tests could be indicative of unatrual contracture or tight muscles that may be the cause of pain. Hamstring length tests like the 90/90, can be used, or the Thoms test to examine quadriceps length. The adjusted Thomas test can also detect iliotibial band tightness.
Nerves should also be examined, through neural provocation tests. Femoral, sciatic, peroneal and other conditions may be eliciting refered pain. Neural tension tests of the lower limb, involve movement in the neck, as we stretch the specific nerve through the lower leg, in order to detect different levels of neural mechanisms that may be reffering pain to the knee.
Author:
Constantinos Hadjichristofis – Bcom HRM (Wits) PT (ACSM) BSc (Hons) Physiotherapy (Herts) MSc – Sports Medicine, Exercie and Health (UCL).